









Charcot arthropathy occurs in the presence of peripheral neuropathy and metabolic abnormalities. Today it is seen more commonly in patients with long-standing diabetes1,2. Its pathogenesis, although still largely unknown, involves several pro-inflammatory pathways, which stimulate osteoclastic activity3.
A rapid and accurate Charcot diagnosis is essential to protect the foot and reduce the chance of further bony collapse of the foot and ankle. However, early-stage Charcot foot is often misdiagnosed, due to three main factors:
- Relative rarity of the condition4
- Absence of clear, defined signs and symptoms5
- Little to no knowledge about the condition from non-specialists6
The last point is particularly relevant in the context of referrals from the general practitioners. Lisa Grant-McDonald, DPM, notes that patients with suspected Charcot are sent to many different specialties, including internal medicine, vascular surgery, and orthopedic surgery. When a misdiagnosis is made, this delays a prompt intervention. Charcot arthropathy treatment strongly benefits from attentive physicians well versed in its treatment and a multidisciplinary approach, where all specialists work together. If you would like to know more about the advantages of having a multidisciplinary health care team, and have some material to give to your patients to help them know more about Charcot arthropathy, please read the article “Charcot Foot and Ankle Diagnosis: The Multidisciplinary Approach.”
The challenges mentioned above often delay the initial treatment of Charcot arthropathy, which can then progress to limb- and life-threatening complications2. In this article, we will focus on the distinguishing features of the early stages of Charcot arthropathy and its symptoms, when the radiographs may still reveal an intact osseous structure.

Early-stage Charcot Arthropathy
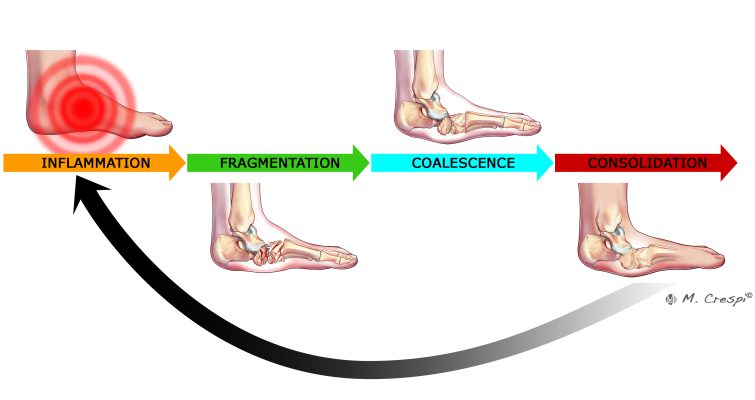
There are four different stages in Charcot foot, often grouped in active versus non-active disease states: inflammation, fragmentation, coalescence, consolidation7. Patients usually only go through one round of the different stages, but approximately 23% of them can suffer through multiple cycles (Figure 1)7,8. An earlier classification developed by orthopedic surgeon Sidney N. Eichenholtz defined the three stages of Charcot arthropathy based on the natural history of the disease. Stage I was the development, stage II the coalescence, and stage III the reconstruction9.
While radiographic imaging is useful in the later stages, it is less so in the inflammatory stage of Charcot, where it often shows no alterations10. If there is a high suspicion of Charcot in its early stages, magnetic resonance imaging (MRI) and bone scans can be useful in detecting bone marrow edema and distinct bone alterations10,11. Tagged white blood cell scans can also be used to differentiate infection from acute Charcot arthropathy12. However, according to the feedback from our interviewed Charcot experts, MRI can be difficult to interpret, given its high sensitivity. Diagnostic imaging, while important, should always be preceded by a careful clinical evaluation of the patient to minimize the risk of misdiagnosis and delayed treatment.
Initial Signs and Symptoms of Charcot Arthropathy
Since there is no single diagnostic test that can unequivocally diagnose Charcot, physical examination is the cornerstone of staging and diagnosing the condition13. All patients with diabetes should be examined at least once a year for potential foot problems, and more often if they have risk factors14.
Early-stage Charcot starts with a red, hot, and swollen foot, with patients frequently complaining that their foot no longer fits into a shoe and is often painful10. The precipitating event is often trauma, such as slipping or twisting, although the patient often may not recall a specific traumatic event10. Pain may or may not be present, due to the sensorial alterations caused by peripheral neuropathy2,15. Since neuropathy is a pre-requisite for the development of Charcot foot, it is useful to confirm its presence by Semmes-Weinstein monofilament or vibratory perception threshold16.
Although peripheral artery disease is common in patients with diabetes, Charcot arthropathy usually presents with exaggerated blood flow which, along with the inflammatory process, leads to increased temperature in the affected foot, about 2–5°C (3.6–9°F)10,16. Some specialists, including Stephanie Oexeman, DPM, are big proponents of thermography. She uses an app to store thermal data from her patients and evaluate how temperature changes over time.
Daniel Scott, MD, MBA (Medical University of South Carolina) also highlights that warmth, redness and swelling are red flags of early Charcot and that thermography is helpful to quantify and document asymmetry in temperature. Furthermore, he mentions a helpful tip to differentiate Charcot foot from infection: in Charcot, the warmth, redness, and swelling improve with elevation, while in infection these signs remain unchanged.
The diabetic foot symptoms that clinicians should be most attentive to are summarized in Table 1.
Sign or symptom |
Assessment |
| Unilateral erythema, ligament laxity, and swelling | Clinical observation |
| Peripheral neuropathy | Semmes-Weinstein monofilament or vibratory perception threshold |
| Increased temperature | Clinical observation or thermal mapping (more accurate) |
| Pain of the affected foot | Patient history |
Misdiagnosis of Charcot Foot
According to a recent systematic review, more than half (53.2%) of Charcot cases involving the foot are initially misdiagnosed, leading to long wait times from symptom onset to correct diagnosis1. Because Charcot of the foot is not at the forefront of most clinicians’ minds, it is often misdiagnosed as skin or bone infections, other inflammatory conditions, fractures, sprains, or deep vein thrombosis1. Foot ulcers, common in diabetic patients, can also create challenges with correctly diagnosing this condition, as worsening deformity from Charcot arthropathy can lead to early ulceration17.
An untimely diagnosis of Charcot of the foot will significantly increase medical treatment costs and health care resource utilization, but most importantly, it will reduce the patients’ quality of life and life expectancy17,18.
In conclusion, a timely and accurate early-stage Charcot arthropathy diagnosis should be a priority for every clinician caring for patients living with diabetes, so that appropriate treatment can be quickly implemented.

References
- Korst GS, Ratliff HT, Torian J, Jimoh RO, Jupiter DC. Delayed Diagnosis of Charcot Foot: A Systematic Review. The Journal of Foot and Ankle Surgery. 2022/09/01/ 2022;61(5):1109-1113. doi:https://doi.org/10.1053/j.jfas.2022.01.008
- Schmidt BM. Clinical insights into Charcot foot. Best Pract Res Clin Rheumatol. Jun 2020;34(3):101563. doi:10.1016/j.berh.2020.101563
- Jansen RB, Svendsen OL. A review of bone metabolism and developments in medical treatment of the diabetic Charcot foot. Journal of Diabetes and its Complications. 2018/07/01/ 2018;32(7):708-712. doi:https://doi.org/10.1016/j.jdiacomp.2018.04.010
- Trieb K. The Charcot foot. The Bone & Joint Journal. 2016;98-B(9):1155-1159. doi:10.1302/0301-620x.98b9.37038
- Marmolejo VS, Arnold JF, Ponticello M, Anderson CA. Charcot Foot: Clinical Clues, Diagnostic Strategies, and Treatment Principles. Am Fam Physician. May 1 2018;97(9):594-599.
- Schmidt BM, Wrobel JS, Holmes CM. Physician knowledge of a rare foot condition – influence of diabetic patient population on self-described knowledge and treatment. Article. Clin Diabetes Endocrinol. 2017;3(1)
- Rosskopf AB, Loupatatzis C, Pfirrmann CWA, Böni T, Berli MC. The Charcot foot: a pictorial review. Insights Imaging. Aug 5 2019;10(1):77. doi:10.1186/s13244-019-0768-9
- Osterhoff G, Böni T, Berli M. Recurrence of acute Charcot neuropathic osteoarthropathy after conservative treatment. Foot Ankle Int. Mar 2013;34(3):359-64. doi:10.1177/1071100712464957
- Rosenbaum AJ, DiPreta JA. Classifications in brief: Eichenholtz classification of Charcot arthropathy. Clin Orthop Relat Res. Mar 2015;473(3):1168-71. doi:10.1007/s11999-014-4059-y
- Rogers LC, Frykberg RG. The Charcot Foot. Medical Clinics of North America. 2013/09/01/ 2013;97(5):847-856. doi:https://doi.org/10.1016/j.mcna.2013.04.003
- Ahluwalia R, Bilal A, Petrova N, et al. The Role of Bone Scintigraphy with SPECT/CT in the Characterization and Early Diagnosis of Stage 0 Charcot Neuroarthropathy. J Clin Med. Dec 21 2020;9(12)doi:10.3390/jcm9124123
- Lauri C, Glaudemans A, Campagna G, et al. Comparison of White Blood Cell Scintigraphy, FDG PET/CT and MRI in Suspected Diabetic Foot Infection: Results of a Large Retrospective Multicenter Study. J Clin Med. May 30 2020;9(6)doi:10.3390/jcm9061645
- Abyar E, McKissack H, Johnson MD. Chapter 19 – The surgical management of the Charcot foot: physical examination of the foot prior to surgery, indications and criteria for amputation, and surgical techniques. In: Pierre-Jerome C, ed. The Essentials of Charcot Neuroarthropathy. Elsevier; 2022:441-448.
- Apelqvist J, Bakker K, van Houtum WH, Schaper NC. Practical guidelines on the management and prevention of the diabetic foot. https://doi.org/10.1002/dmrr.848. Diabetes/Metabolism Research and Reviews. 2008/05/01 2008;24(S1):S181-S187. doi:https://doi.org/10.1002/dmrr.848
- Rogers LC, Frykberg RG, Armstrong DG, et al. The Charcot Foot in Diabetes. Journal of the American Podiatric Medical Association. 01 Sep. 2011 2011;101(5):437-446. doi:10.7547/1010437
- Rogers LC, Bevilacqua NJ. The diagnosis of Charcot foot. Clin Podiatr Med Surg. Jan 2008;25(1):43-51, vi. doi:10.1016/j.cpm.2007.10.006
- Labovitz JM, Shapiro JM, Satterfield VK, Smith NT. Excess Cost and Healthcare Resources Associated With Delayed Diagnosis of Charcot Foot. The Journal of Foot and Ankle Surgery. 2018/09/01/ 2018;57(5):952-956. doi:https://doi.org/10.1053/j.jfas.2018.03.036
- van Baal J, Hubbard R, Game F, Jeffcoate W. Mortality Associated With Acute Charcot Foot and Neuropathic Foot Ulceration. Diabetes Care. 2010;33(5):1086-1089. doi:10.2337/dc09-1428




