







Surgical reconstruction of foot and ankle Charcot with external fixation is especially useful in the presence of poor bone quality, ulceration, compromised soft tissue, active infection, or osteomyelitis – cases in which the use of internal fixation is limited or contraindicated1.
This article will review the main indications and benefits of external fixators, describe the different external fixation options for Charcot foot reconstruction, and will discuss challenges, complications, and considerations for postoperative management.
Indications for External Fixators
External fixators have many advantages for treatment of foot and ankle Charcot. Whereas internal fixation is contraindicated in patients with suspected infection, external fixation has the advantage that fixation wires can be inserted proximal and distal to potentially infected joints and then later removed2. In patients with severely destructed bone, external fixation is beneficial as it does not rely on cortical purchase for stabilization, and bone quality is less critical3. It can be applied with minimal soft tissue dissection and preserves osseous vascular supply3. When necessary, surgeons can address large bone defects with bone transport via the external fixator3. One of the main benefits for the patient is the possibility of earlier weightbearing compared to internal fixation3. According to a recent consensus statement of Charcot foot experts, external fixation is almost always required in the presence of deformity, open wounds, or active infections4.
“External fixation is the treatment of choice in the presence of infection, especially with deep infections, such as septic joints. External fixation can be followed by internal fixation when the frame is removed after about 3 months and the foot is still not stable.” (Mohammad Sharif, DPM, Village Podiatry, Atlanta)
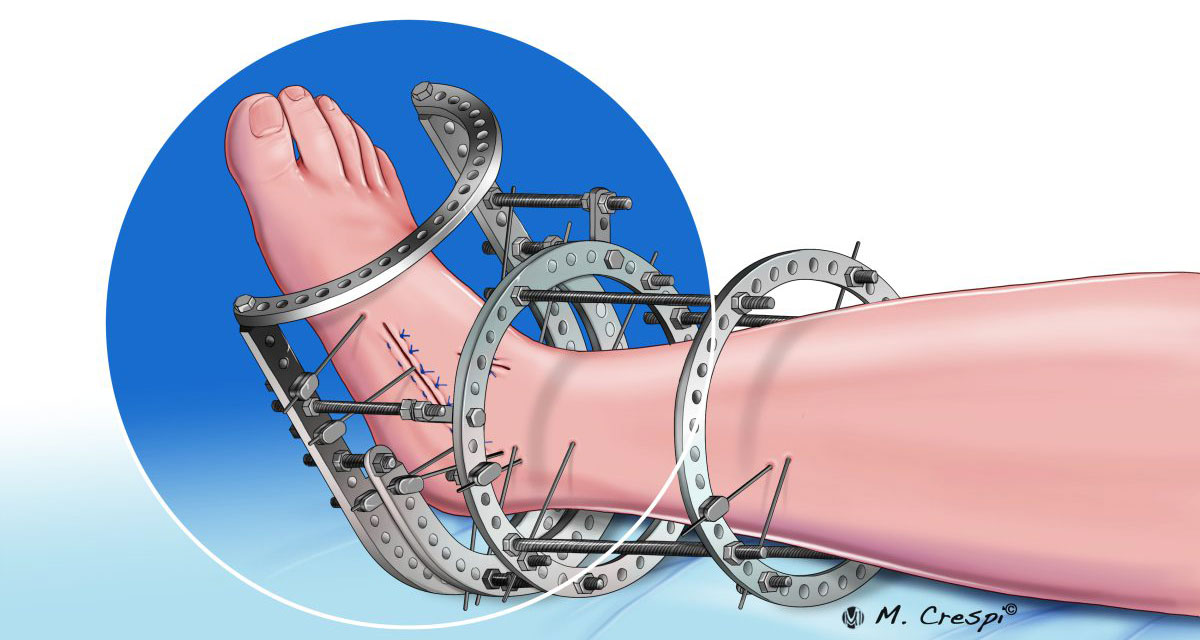
Circular Fixators
Circular fixators are the most commonly used constructs for external fixation, as they enable deformity correction while providing stability and compression when arthrodesis is required5. Compared to monolateral external fixators, circular fixators do not rely on the cortical fixation of half pins but gain stability through transosseous wires5. Circular fixators consist of rings surrounding the tibia and foot which are suitable for addressing deformities of the foot and ankle5. Different circular fixation constructs are either static or dynamic or focus on stabilization for offloading5,6:
- Static circular fixation provides primary stability and can augment fixation5. Surgeons can prebuild the frame for easier application5.
- Dynamic circular fixation is beneficial for severe deformities requiring staged correction with a reduced risk for over- or undercorrection5.
- Offloading constructs are useful to promote wound healing and for soft tissue reconstruction5. They provide continued access to local wound care and can be converted to a static or dynamic circular fixation construct5.
Hexapod Fixators
Hexapods are circular frames consisting of external supports, known as rings and footplates, connected by six struts that span the level of the deformity and allow for multiplanar deformity correction. The frame is attached to the bone via thin wires or half-pins. This construct allows multiplanar adjustments.
“I use hexapod external fixators a lot for deformity corrections as they allow for dynamic treatment and can ‘move’ the bone in a more appropriate position”, says Lisa Grant-McDonald (DPM, Doctors Grant Foot & Ankle, Virginia Beach).
The following case report shows how a hexapod frame was used in a two-stage correction of a complex Charcot foot deformity. The patient presented with soft tissue dislocation that had been present for 10 months. Figure 1 shows the right foot with equinus, valgus, 48 degrees abductus with 22 mm lateral translation.

If available, software planning tools can be used for detailed deformity correction. In this case, a Miter frame (two TL-HEX stacked frames sharing the central ring) was used separately to address the hindfoot equinus and valgus. The foot portion was to correct the abductus and translation via a midfoot percutaneous Gigli saw osteotomy. After 9 weeks, the Mearys angle was realigned to 0°.
Postoperative pictures
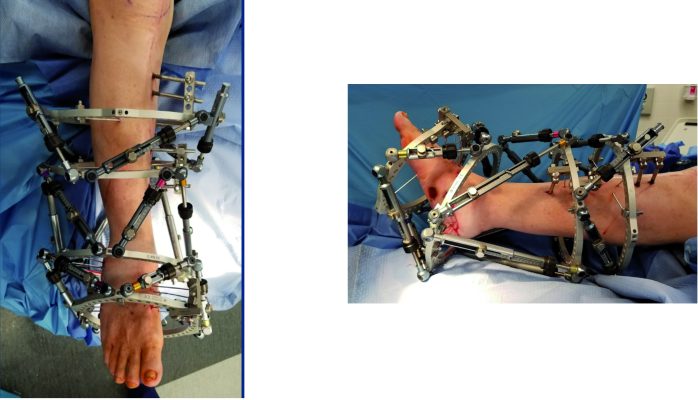
The patient underwent midfoot beaming of the medial and lateral columns in the second stage. The two-stage approach resulted in a plantigrade foot without requiring revision surgery. For more information about this case, including follow-up X-rays and images of the final result, you can download the full report here.
Combination of Internal and External Fixation (Superconstructs)
Patients with Charcot foot deformities require a highly individualized treatment approach7. Combined internal and external fixation is often the preferred technique for complex foot or ankle Charcot reconstructions in the severely deformed foot7. In this approach, circular fixators can stabilize adjacent joints if needed7. When plastic surgery is required to close open wounds after ulcer excision, the external fixator can be used to offload the flap or skin graft7. Circular fixators also serve as an additional deterrent for inappropriate weightbearing or can allow for early weightbearing7. Internal fixation allows appropriate alignment of the deformity and compression for fusion1. Overall, the combined approach provides both stability and compression across the arthrodesis site.
This is also confirmed by Stephanie Oexeman (DPM, Oexeman Foot & Ankle, Chicago): “Superconstructs are particularly suitable for larger and obese patients who are not able to avoid weight-bearing. That’s why it is so important to keep the patient’s history in mind.”
Daniel Scott (MD, MBA Medical University of South Carolina (MUSC) Orthopaedics, Charleston) also uses the combined approach for complex cases: “Difficult conditions such as Charcot ankle can be treated by combining a tibiotalocalcaneal nail with external fixation to address the complex deformity and allow for earlier weightbearing and better rates of clinical success.”
Complications
The most common complications associated with external fixation are pin site infections, pin/wire fixation failure, deep infection, malunion or nonunion, and psychological complications due to the device5,7. Besides surgical experience, the outcome also highly depends on appropriate patient selection, continuous patient education, family support, and regular follow-up by a multidisciplinary team5.
Considerations for Postoperative Care
In general, patients treated with external fixators require a more frequent follow-up than patients treated with isolated internal fixation.
Daniel Scott (MD, MBA Medical University of South Carolina (MUSC) Orthopaedics, Charleston) explains his follow-up approach: “Patients treated with a circular frame require follow-up every 2 weeks to monitor pin site infections and allow for early detection of any complications with the frame. Less frequent visits are required after frame removal when patients ambulate with a walking cast or boot. For internal fixation, sutures are usually removed after 2 weeks, followed by monthly visits.”
The appropriate approach to take for postoperative care can be controversial, especially regarding immobilization. For patients with external fixators, more frequent follow-ups should be considered to monitor for pin site infections. Routine radiographs should be considered at 6 weeks, 3 months, and every 3 months until bone union is clearly evident8.
Further Reading
Download the Charcot foot surgical cases available for more information about external fixation for Charcot foot reconstruction.

References
1. Brandão RA, Weber JS, Larson D, et al. New Fixation Methods for the Treatment of the Diabetic Foot: Beaming, External Fixation, and Beyond. Clin Podiatr Med Surg. Jan 2018;35(1):63-76. doi:10.1016/j.cpm.2017.08.001
2. Giurini J. A Closer Look at Fixation Options for the Charcot Foot. Podiatry Today; 18(11). 2005;
3. Schade VL, Andersen CA. A literature-based guide to the conservative and surgical management of the acute Charcot foot and ankle. Diabet Foot Ankle. 2015;6:26627. doi:10.3402/dfa.v6.26627
4. Salvaterra P. The Surgical Management of Neuropathic (Charcot) Foot – A Practical Guideline. 2017;
5. Stapleton JJ, Zgonis T. Surgical reconstruction of the diabetic Charcot foot: internal, external or combined fixation? Clin Podiatr Med Surg. Jul 2012;29(3):425-33. doi:10.1016/j.cpm.2012.04.003
6. Pinzur MS. The role of ring external fixation in Charcot foot arthropathy. Foot Ankle Clin. Dec 2006;11(4):837-47. doi:10.1016/j.fcl.2006.06.006
7. Capobianco CM, Ramanujam CL, Zgonis T. Charcot foot reconstruction with combined internal and external fixation: case report. J Orthop Surg Res. Feb 11 2010;5:7. doi:10.1186/1749-799x-5-7
8. Alrashidi Y, Hügle T, Wiewiorski M, Herrera-Perez M, Valderrabano V. Surgical Treatment Options for the Diabetic Charcot Midfoot Deformity. Clin Podiatr Med Surg. Jan 2017;34(1):43-51. doi:10.1016/j.cpm.2016.07.006




