











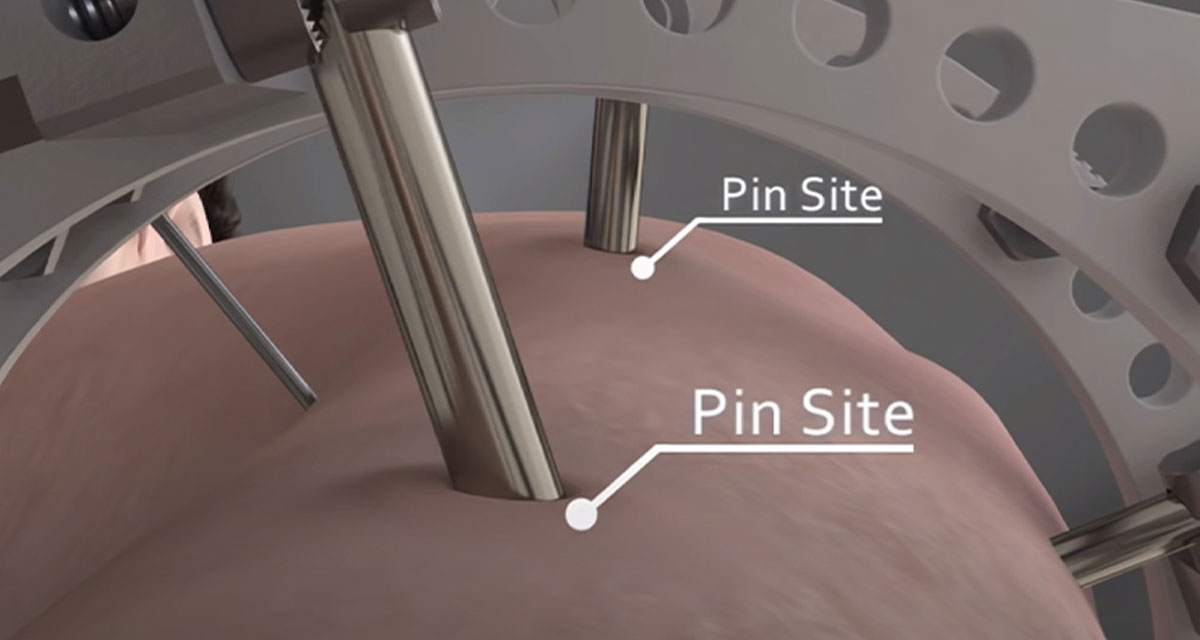
Preserving healthy pin sites is essential to effective external fixation, for the prevention of pin track infection and related complications. All people involved in the healing process – general practitioner, surgeon, nursing staff, patient and family – play a fundamental role in order to achieve the best result. Here are some useful key points.
Healthy pin sites depend on both an excellent surgical technique for screw insertion during the intra-operative phase, and accurate pin site care during the post-operative phase.
In the operating theatre, wire and pin insertion should be as low energy and atraumatic as possible, with minimum damage to the skin, soft tissue and bone.(1) After completion of the inserting procedure, all pin sites must be free of skin tenting and soft tissue impingement.(2)
Regarding the post-operative period, there is no universally accepted protocol for the optimal care of pin sites. The standard Orthofix guidelines on post-operative pin sites care have been based on the valuable work done by a surgeon and a nurse at the Sunderland Royal Hospital, United Kingdom – Mr. R. Checketts and Sister M. Otterburn.(3) This technique, which has stood the test of time, requires regular cleaning of the screw shanks and surrounding skin with sterile water, always using new sterile cotton buds for each screw; maintaining the skin mobile around the screw; and preventing skin tethering by means of skin releases as required.
Here follow some key points for surgeons for healthy pin sites:
- Blunt dissection down to the bone, splitting the soft tissues to allow insertion of the screw guide up to the bone, avoiding tethering of the screw by the deep structures;
- Ensure that the screw clamp is tightened around the screw guides, so that screws are inserted perfectly parallel to one another;
- Always utilize sharp drill bits, and destroy blunt ones to avoid recycling;
- Always irrigate screw sites with saline solution after screw insertion, removing all bony fragments;
- Always check for skin or fascial tethering at the end of surgery. Perform skin or fascial releases as necessary;
- Clean screw shanks, fixator and surrounding skin. If using an antiseptic, this should not come in contact with the black parts of the aluminium fixators;
- During half-pin insertion, ensure pin cooling, using a stop-start modality when drilling and continuous irrigation with cold saline, and a non-touch technique as far as possible.(4)
The patient, together with all people involved in the healing process, should be informed of the protocol they need to follow for pin site during the post-operative phase.
References
- Ferreira N, Marais LC 2012. Prevention and management of external fixator pin track sepsis. Strategies Trauma Limb Reconstr; 7(2):67-72.
- Bibbo C, Brueggeman J 2010. Prevention and management of complications arising from external fixation pin sites. J Foot Ankle Surg; 49:87-92.
- Checketts RG, Otternburn M et al. 1993. Pin Track infection: definition, incidence and prevention. Suppl Int J Orth Trauma; 3(3):16-8.
- Davies R, Holt N , Nayagam S 2005. The care of pin sites with external fixation. J Bone Joint Surg; 87-B:716-9.




