











The Orthofix history began at the end of the 70s in Italy with the work of orthopedic researcher Giovanni De Bastiani. He proposed the concept of “dynamization” and developed a modular external fixation device designed to allow the release of axial forces at the proper time during the healing process, thus transferring a progressive load to the fracture site. After this first device, other devices were developed by Orthofix to better satisfy patients’ and doctors’ needs.
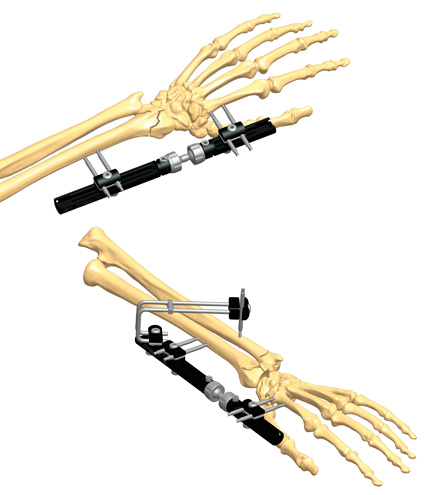
The original device, named DAF (Dynamic Axial Fixator), had a telescopic body, consisting of two parts, one sliding in an axial direction within the other. The two components were locked together by tightening a central body locking nut to create one rigid unit immediately after the initial application of the device. This rigidity had to be maintained until the decision was taken to dynamize the fracture.
Prof. De Bastiani advocated commencement of dynamization when some evidence of callus was seen in the radiographs, generally after 2-6 weeks, in a stable fracture. This indicates the phase of hard callus formation, when bony union has generally reached enough strength and rigidity for the patient to recover cautious function.(1) (2) (3) That is why for some experts the term dynamization might equate more to dynamic axial loading, with closure of the fracture gap, than to dynamic axial motion.
Clinical studies initially showed highly encouraging results when applying DAF, associated with a low incidence of pin track infection and non-union rate.(4) DAF did provide cyclic axial micromotion – during patients’ walking on the locked frame and cautious weightbearing – as well as later progressive loading, thus allowing for the most appropriate and beneficial kind of applied movement at each stage of the healing process.
Gradual understanding of the concept of dynamization in all its aspects lead to improvement of the DAF design – with the introduction of crucial changes – and pushed the development of new types of external frames, able to respond to the different needs of surgeons and patients.
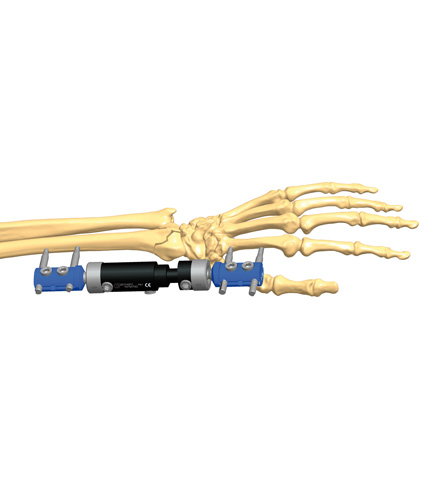
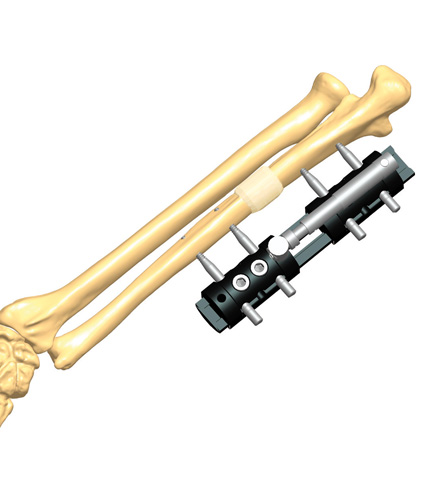
The “Dyna-Ring attachment” was developed to guarantee no more than 2mm of early motion, when in case of very comminuted fractures, in which the risk of collapse and shortening is generally high. Later the “ProCallus Fixator” was thought to allow a more reliable and controlled cyclic micromotion, to be applied at an earlier stage of the healing process, even before the patient was capable of partial weightbearing. Compared to the DAF, this device still consists of two parts, but now they slide one against the other in a groove, rather than fitting one inside the other. A cyclic micromotion up to 2mm is made possible by a spring-loaded micromotion facility which functions with the central body locking nut tightened and the micromovement locking nut loosened. This controlled cyclic micromovement can be applied even when the patient is still confined to bed by using the “Actuator”. The physiological requirements to correctly perform dynamization with the ProCallus fixator during all phases of the fracture healing process were then synthesized in a protocol which links action to appropriate timing.
References
- De Bastiani G, Aldegheri R et al. 1984. The treatment of fractures with a dynamic axial fixator. J Bone Joint Surg; 66B:535-45.
- De Bastiani G, Aldegheri R et al. 1986. Dynamic Axial fixation. A rational alternative for the external fixation in fractures. Int Orthop; 10:95-9.
- Frost HM 1989. The biology of fracture healing. An overview for clinicians. Part I. Clin Orthop; 248:283-93.
- Wallace WA, Howard PW 1993. A Decade of Tibial Shaft Fractures. Int J Orthop Trauma; 1993 (Suppl.III): 61-63.




