
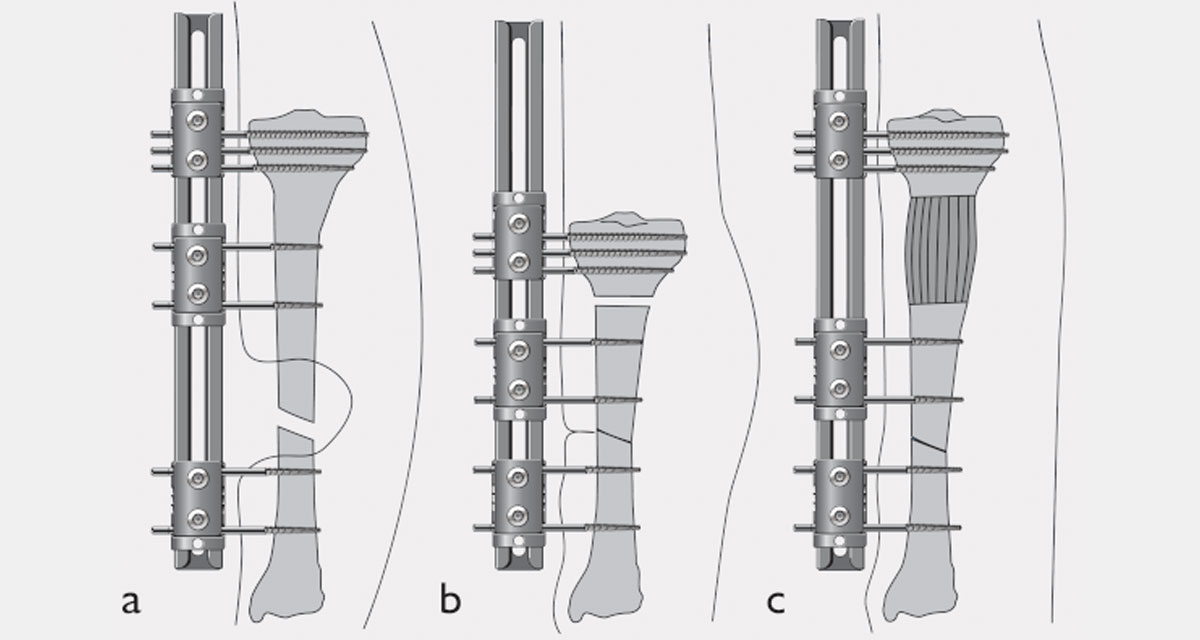
In the compression-distraction technique, one site of the bone is lengthened and another site is immediately or gradually compressed. In the lower limb, the compression-distraction technique is generally performed in the presence of leg shortening associated with small bone defects – less than 3cm in the tibia and/or less than 5cm in the femur.
The compression-distraction technique may also be used for shortening associated with a diaphyseal deformity – angulated nonunion or malunion – since the diaphyseal bone is less suitable for lengthening. The deformity is corrected at the diaphyseal osteotomy site, while lengthening (distraction) is performed at the metaphyseal osteotomy site. In infected cases, this technique may be suitable to close the bone defect and delay lengthening until infection is under control. When performing this technique, surgery should be the natural consequence of a very precise preoperative planning. Shortening – acute or gradual – must always be performed with constant monitoring of the venous and arterial circulation.
The choice of the device to be applied depends on the type and severity of the nonunion or malunion. When applying the external fixator, tension of soft tissues potentially caused by the bone fixation elements in both longitudinal and transverse directions must be avoided. Stability is a crucial point for a successful treatment, as well as prevention of post-operative joint stiffness, by maintaining the correct position of the joint when inserting the bone fixation elements in proximity of the joint. Therefore, with external frames particular attention must be given to the proximity of the knee and ankle joints: screws and wires should not be applied at distances less than 15mm from the knee joint or less then 12mm from the ankle joint, in order to obtain safe and extracapsular application.(1) Another good reason to strictly adhere to the previously planned surgical program is related to possible future frame adjustments. With the Ilizarov-type ring fixators, where the rods go through the rings’ holes, it is important that the rings that could be needed in the future are inserted in the original structure – for instance, in the case of bifocal compression-distraction osteosynthesis.(2)
Best treatment is prevention, which is substantially based on two golden rules: the first one, avoid necrosis of the tissue – which can be provoked during the insertion of screws and wires by producing overheat, and avoid the excessive tension of soft tissues – which may be caused by a wrong technique of insertion, or an incorrect connection to the external frame followed by straining in flexion of the wire or screw. The second rule, avoid excessive motion of the tissues around the bone fixation elements due to an unstable mounting. Knee stiffness can be prevented by correctly positioning the knee when inserting wires and screws – usually they go through the flexor muscle with the knee extended, and through the extensor muscles with the knee flexed.(3)
References
- De Coster TA, Crawford MK et al. 1999. Safe extracapsular placement of proximal tibia transfixation pins. J Orthop Trauma; 13:236-40.
- Mazzarello F, Puncuh F et al. 1997. Limb external devices application: anesthetic procedures comparison. Gaslini; 29:55-60.
- Mora R, Bertani B et al. 2006. Compression-Distraction Methods, in: Mora R (ed). Non union of the Long Bones. Milano: Springer; pp. 89-117.




