
Bone transport is a surgical technique that allows regeneration of bony tissue when there are defects in the bone caused by fractures, non-unions, chronic bone infections, or tumors. In such cases, bone regeneration is used to fill a gap or a piece of missing bone. There are several bone transport techniques depending on the location and size of bone defect.(1)
With the classic bone transport technique, an osteotomy (or a corticotomy) is performed in the bone and an external fixator is used to transport the bone, thereby promoting the development of new bone to fill the gap. Bone transport is performed when the bony defect is more than 3 cm in the tibia and 5 cm in the femur (classified as intermediate or large defect). Bone transport technique differs from lengthening because instead of the bone and soft tissues keeping a relatively fixed relationship, the bone slides in the soft tissue envelope similarly to a lift inside a shaft.
One week after the osteotomy, bone transport begins at a rate of 0.75 to 1 mm per day. Slow transport of one or more bony segments is accomplished by gradually moving a bony segment from one position to another. The process of bone formation in the distraction site is known as distraction osteogenesis. In the bone transport technique, the transported segment moves to fill the bone defect. Attentive monitoring of segmental bone transport in needed to prevent the risk of misalignment, infection and joint deformities.(2) Once bone transport is complete and the two bone segments are in contact, union may be reached by compression, with the resection of bony ends and compression, with bone grafting, or various other ways.
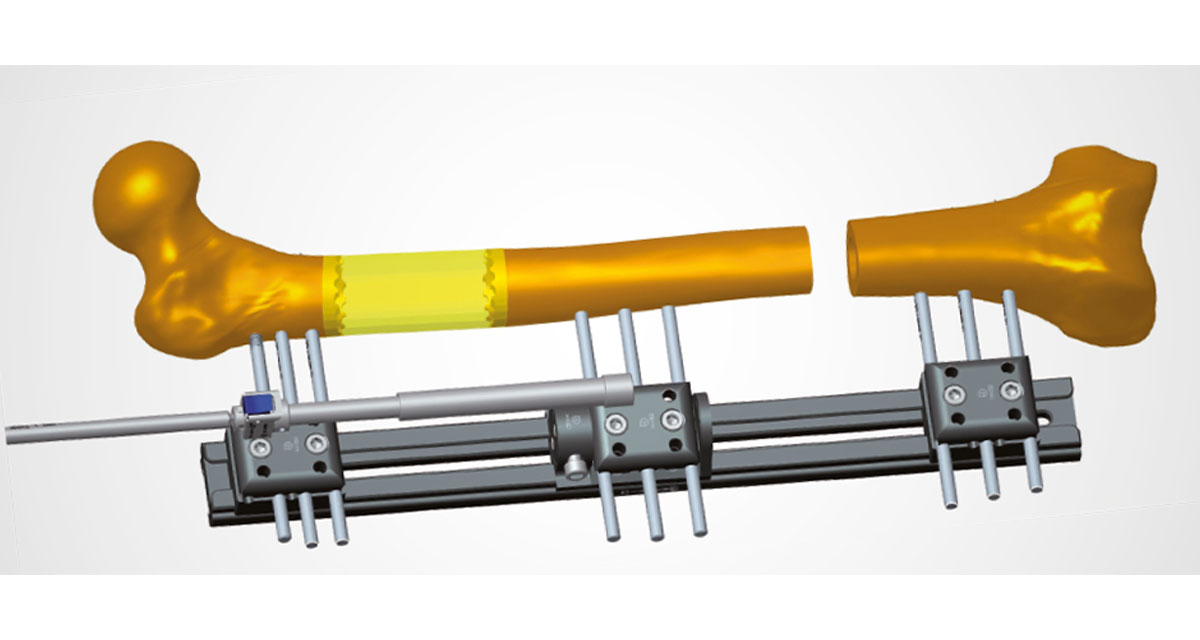
When an external fixator is used for the bone transport, the proximal and distal bone segments are stabilized with screws and/or wires, which are fixed to the external frame. If a circular frame is used, the wires and/or screws will be fixed to a ring, and if a monolateral frame is used, they will be fixed to a clamp. The middle bone segment will be fixed to an intermediate ring or clamp. After the osteotomy, this middle segment is gradually moved towards the bone defect.
The use of a monolateral external fixator to perform bone transport was described by Prof. De Bastiani from the University of Verona. His technique, called callotasis, implies the gradual symmetrical distraction of the developing callus following a corticotomy through the controlled movement along the monolateral external fixator. The biological response to this technique is similar to that described by Prof. Ilizarov in association with circular external frames.(3,4)
Recently, hybrid bone transport techniques have been developed, in an effort to improve patient comfort and reduce complications associated with the prolonged use of an external fixator.(5) The use of an intramedullary nail after the bone transport allows for early removal of the external fixator, while maintaining the necessary support to the bony regenerate while it consolidates. The intramedullary nail can also be in place for the entire duration of treatment, providing additional rigidity to the fixation and maintaining alignment of the bone segments.
The latest developments in the bone transport technique employ only internal fixation for the entire bone transport treatment, from distraction to consolidation, with the use of motorized intramedullary nails.(5,6) These rigid constructs are composed of 2 telescoping parts, which lengthen when activated by a motorized drive, thus allowing an accurate control of the distraction rate.(7) The application of motorized intramedullary nails for bone transport should be done by experienced surgeons, who should evaluate carefully the patient’s anatomical situation before performing the osteotomy and reaming the intramedullary canal. An important aspect is the use of straight and rigid reamers, as opposed to the flexible reamers that will follow the path of least resistance. This is because the axis alignment and implant position cannot be changed postoperatively, making preplanning a key part of bone transport with these devices.(8)
References
- Brinker M, O’Connor D. The Use of Ilizarov External Fixation Following Failed Internal Fixation. Techniques in Orthopaedics. 12/01 2002;17:490-505. doi:10.1097/00013611-200212000-00013
- Rigal S, Merloz P, Le Nen D, Mathevon H, Masquelet AC. Bone transport techniques in posttraumatic bone defects. Orthop Traumatol Surg Res. Feb 2012;98(1):103-8. doi:10.1016/j.otsr.2011.11.002
- Aldegheri R, Renzi-Brivio L, Agostini S. The callotasis method of limb lengthening. Clin Orthop Relat Res. Apr 1989;(241):137-45.
- Saleh M, Donnan L. The Technique of Callotasis and its Application to Monofocal Limb Lengthening. In: De Bastiani G, Apley AG, Goldberg A, eds. Orthofix External Fixation in Trauma and Orthopaedics. Springer London; 2000:458-466.
- Seng DWR, Oh C-W. Critical size bone defects managed with modern techniques of bone transport: An update. Injury. 2024/03/01/ 2024;55(3):111341. doi:https://doi.org/10.1016/j.injury.2024.111341
- Chimutengwende-Gordon M, Mbogo A, Khan W, Wilkes R. Limb reconstruction after traumatic bone loss. Injury. 2017/02/01/ 2017;48(2):206-213. doi:https://doi.org/10.1016/j.injury.2013.11.022
- Singh S, Lahiri A, Iqbal M. The results of limb lengthening by callus distraction using an extending intramedullary nail (fitbone) in non-traumatic disorders. Article. Journal of Bone and Joint Surgery – Series B. 2006;88(7):938-942. doi:10.1302/0301-620X.88B7.17618
- Krieg AH, Speth BM, Foster BK. Leg lengthening with a motorized nail in adolescents: an alternative to external fixators? Clin Orthop Relat Res. Jan 2008;466(1):189-97. doi:10.1007/s11999-007-0040-3




