


The term CORA (Center of Rotation of Angulation) means a method of mechanical and anatomical axis planning based on joint orientation, which has gained international recognition and acceptance. Many surgeons from all over the world apply this method to limb lengthening and deformity correction, and the CORA principles and concepts have clearly shaped both design and functionality of the last generation of external devices.
The CORA (Center of Rotation of Angulation) is both a method of mechanical and anatomical axis planning based on joint orientation and a system of deformity analysis that is applicable to any current osteotomy techniques and hardware. The CORA method of deformity analysis initially began with reference to the Ilizarov ring fixators, as an attempt to understand what made this type of device so effective and unique in its ability to correct deformities in a controlled modality. However, the aim was also to understand what caused some of the secondary deformities that arose from mismatching the location of the Ilizarov hinge and the CORA.(1)
This effort of understanding and analysis ended up in recognizing that the concept of CORA and the osteotomy rules were not unique to the Ilizarov fixator but universally applicable to deformity correction by any method. The basic principles of analysis and planning are the same regardless of the type of fixation selected. With the CORA method, which allows us to analyze, understand and quantify the deformity, the surgeon can plan surgery for any deformity.
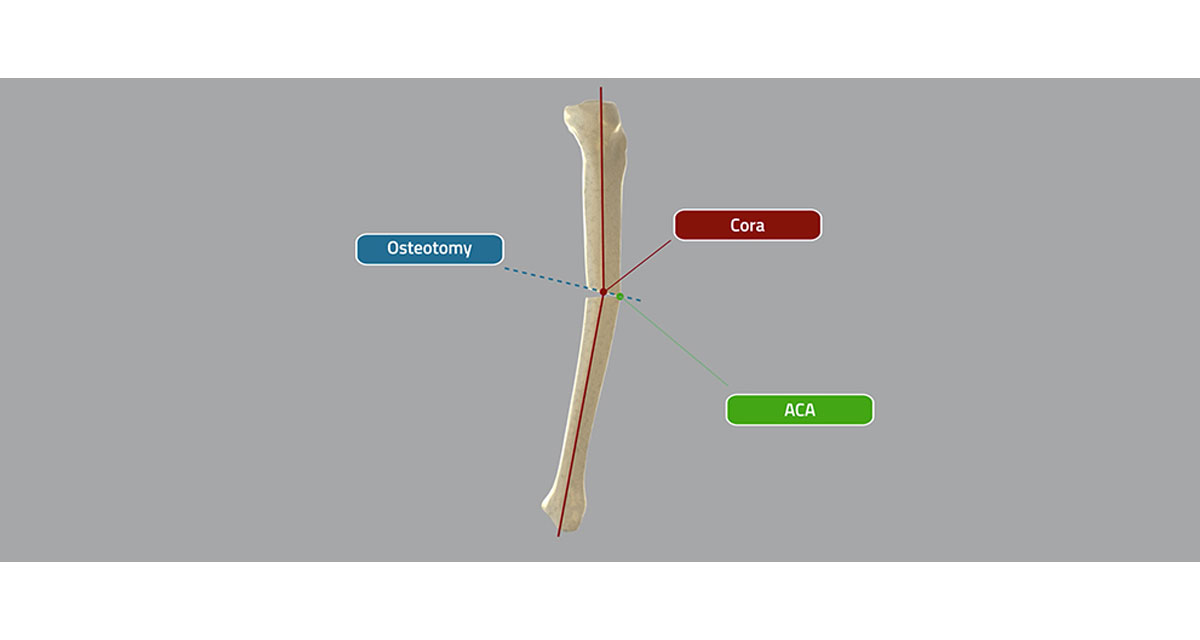
The CORA is quite simple to determine in a deformed tibia, as the mechanical axis on both side of the deformity’s apex is drawn along the center of the diaphysis. If the anatomical axis of each bone segment of a deformed bone is drawn on an X-ray, the lines will intersect, and this is the CORA.
In a deformed femur the CORA is not so practical to determine: the mechanical axis of the proximal femoral segment is generally figured to be a line passing through the center of the femoral head, at right angles to a line from the center of the head to the tip of the greater trochanter, where the distal segment’s axis can be found by considering the axis of the tibia in a retrograde direction, unless there is a deformity at the knee joint level.
The CORA method is considered a work in progress, and some experts have recently proposed new methods for deformity planning.(2) The CORA method has been recently incorporated into the latest computer planning software, but even the mathematical modeling of six axis deformity correction is first dependent on the surgeon’s competence to understand, analyze and quantify the radiographic deformity. These considerations make the CORA method still valid and complementary with the latest computer based methods.
References
- Herzenberg JE. Preface, to: Paley, D. 2002. Principles of Deformity Correction. Berlin Heidelberg New York: Springer-Verlag; p. X.
- Fabricant PD, Camara JM et al. 2013. Femoral deformity planning: intentional placement of the apex of deformity. Orthopedics; 36(5):e533-7.