Charcot Neuropathy in the Diabetic Foot:
Incidence, Causes, Symptoms and Diagnosis
Charcot Neuroarthropathy (CN) is a condition that can occur in people with diabetes who have significant neuropathy. If left untreated, CN may lead to foot deformity, ulceration, infection, amputation, disability and possible premature death. Timely diagnosis and treatment could prevent amputation and long-term disability. Increasing awareness is fundamental to improve CN management and reduce its complications.
Are you a patient? Go to limbhealing.com

HOW SERIOUS
IS CHARCOT FOOT AND
ANKLE DISEASE?

WHAT DOES CHARCOT FOOT
LOOK LIKE AND WHY DOES
IT OCCUR?

HOW IS CHARCOT FOOT
AND ANKLE DIAGNOSED?

THE IMPORTANCE OF
A MULTIDISCIPLINARY
APPROACH

HOW TO PREVENT CHARCOT
FOOT AND ANKLE

CHARCOT
DEFORMITY
ULCER
INFECTION
AMPUTATION
INACTIVITY
POSSIBLE PREMATURE DEATH
WHO ARE MORE LIKELY TO DEVELOP A CHARCOT NEUROARTHROPATHY?

Charcot patients are more likely
to be men

Over 50 years
as average
is the incidence rate of Charcot in
patients with diabetes
How serious is Charcot Foot and Ankle disease?
According to the International Diabetes Federation (IDF), diabetic foot and lower limb complications are an important cause of morbidity, affecting 40 to 60 million people with diabetes worldwide.
Complications from diabetic feet, including ulceration and Charcot Foot and Ankle, are a leading cause of hospitalization, resulting in high disease burden, poor quality of life, and increased healthcare costs.
- Diabetes is the seventh leading cause of death in the USA
- 0.3 to 7.5% of diabetic patients may develop a Charcot Neuroarthropathy
- Almost 100,000 patients with diabetes will suffer an amputation each year in the USA
- Worldwide 85% of leg amputations are a result of a diabetic foot ulcer
- With Charcot Neuroarthropathy, a minor injury can lead to amputation
- Up to 80% of diabetic patients are more likely to die within 5 years of having a limb amputation
Still, with timely diagnosis and appropriate treatments, it is possible to prevent 4 out of 5 amputations. Understanding the diabetic foot and taking the appropriate measures to detect and treat complications as soon as they arise go a long way in the prevention of limb amputation in patients with diabetes.

What does Charcot Foot and Ankle look like?
The name “Charcot Foot” comes from Jean-Martin Charcot – a French neurologist often referred to as one of the world’s pioneers of neurology – who described this condition in 1868.
Charcot Neuroarthropathy is a condition causing weakening of the bones and ligaments in the foot and the ankle that can occur in people who have significant nerve damage (neuropathy), most often related to diabetes. Patients’ ability to feel temperature, pain or trauma decreases.
The bones are weakened enough to fracture and/or dislocate and, with continued walking and weight bearing, the foot eventually changes shape.
As the disorder progresses, the joints collapse and the foot takes on an abnormal rocker bottom shape.
The natural course of Charcot Neuroarthropathy encompasses active and inactive disease phases, which relate to an inflamed or stable disease, respectively. After the consolidation phase, there is a 23% risk of “re activation” of the inflammation phase, which leads to a progressively worse condition.
Charcot Foot and Ankle patients need immediate treatment, as they may develop severe foot and ankle deformity, foot ulcers, infections, disability, gangrene and (worst case scenario) require amputation of the foot.
Why does Charcot Foot and Ankle occur?
Charcot patients are more likely to be men, over 50 years as average
age, with a long history of diabetes, nerve damage to their feet
(diabetic neuropathy) and poorly controlled blood sugar levels.
Lifestyle, such as long-term alcohol, smoking or other substance
abuse, can also increase the risk of developing Charcot Foot Disease.
Charcot Foot typically develops over time and requires a number of
factors to occur. The triggering event for an active stage of Charcot
Foot and Ankle in a susceptible patient can be a sprain, a twisted a
nkle, or even just the load of weight-bearing (especially if the
individual is obese). This starts an inflammatory process, leading to an
osteolysis that is indirectly responsible for the progressive fracture
and deformity.
The role of other factors, such as the reduction of calcitonin
gene-related peptide caused by nerve damage and pre-existing
low bone mineral density, may also be relevant in the
development of Charcot Foot and Ankle.


How is Charcot Foot and Ankle Diagnosed?
Timely and accurate diagnosis is key
The natural course of Charcot Foot and Ankle is characterized by four stages, and the patient can cycle through them in a pattern resembling active and inactive phases, resulting in high morbidity and accentuated foot deformity.
Making an accurate Charcot Foot diagnosis in the early stage of the disease might be difficult, since the acute symptoms can be similar to other conditions, such as cellulitis, gout, or deep vein thrombosis.
Notably, less than one-third of physicians recognize the signs of diabetes-related peripheral neuropathy and diabetic foot problems, even when the patient is symptomatic. The best safeguard is a high index of suspicion, especially in any diabetic patient with a swollen, red, warm foot in the presence of somatic or autonomic neuropathy.
When dealing with Charcot Foot Disease, a timely diagnosis is crucial to improve patient outcomes, facilitate treatment and decrease long-term disability.

What to ask your patient
- Do you have a history of diabetes?
- If yes, do you regularly check your glycemic levels?
- Do you have a history of diabetic foot pathology?
- Did you have prior angioplasty, stent or leg bypass surgery?
- Do you feel any leg or foot pain and discomfort at rest?
- Have you noticed a loss of your leg sensation?
- Has your foot lost the ability to feel pain, heat and cold?
- Do you smoke?
- Do you drink alcohol?

What to look for
- Warm, swollen, red foot and/or ankle (Active Charcot)
- Higher temperature of 2°C or 4°F of one foot compared with the contralateral one
- Interdigital maceration
- Skin lesions, ulcers and open wounds
- Hypertrophic calluses or corns
- Discolored, ingrown nails
- Crepitant cellulitis
- Fungal infection
- Bone deformities
- Loss of foot sensitivity
- Limited range of joints motion
- Absence of Achilles Tendon reflex
- Vascular compromise, with sudden absence of dorsalis pedis and posterior tibial pulses
- Peripheral arterial disease
- Diabetic gangrene and necrosis
- Previous amputation

What to teach your patient
- Have a preventive foot evaluation every year
- Examine foot skin and nails daily and have a regular expert podiatric care
- Report any swelling, redness, lesions and skin discoloration
- Choose appropriate footwear
- Do not walk barefoot
- Replace orthotic shoes every year: they should fit perfectly
- Report absence of pain when it should be felt (e.g. touching hot water)
- Stop or reduce smoking
- Reduce alcohol
Proper surgical procedure is the responsibility of the medical professional. This information is furnished as an informative guideline. Each surgeon must evaluate the appropriateness of a technique based on his or her personal medical credentials and experience.
When is time for a specialist?
Priority
Indications
Timeline
Follow-up
Priority

Indications
- Open wounds and deep ulcers
- Pain at rest
- Active Charcot Foot deformity
(red, hot, swollen) - Vascular compromise
Timeline
- Urgent/immediate referral
- Patient needs interdisciplinary care
management, off-loading with total
contact cast devices and/or surgery,
diabetic orthopedic footwear
Follow-up
- According to specialist decision
Priority

Indications
- No sensitivity
- Ulcers
- Chronic vascular venous insufficiency
- Previous lower limb amputation
related to diabetes
Timeline
- Immediate/first available referral
- Patient needs diabetic orthopedic
footwear, preventative off-loading
and appropriate therapy
Follow-up
- Every 1-2 months
Priority

Indications
- Insufficient sensitivity
- No ulcers
- Foot deformity
- Posterior tibial pulse diminished
or absent - Foot swelling, aedema
Timeline
- No ulcers
- Foot deformity
- Posterior tibial pulse diminished
- or absent
- Foot swelling, edema
- Referral within 3 weeks
- Patient needs prescriptive footwear,
preventative off-loading and
appropriate therapy
Follow-up
- Every 2-3 months
Priority

Indications
- Insufficient sensitivity
- No ulcers
- No foot deformity
Timeline
- Referral within 1 months
- Patient needs prescriptive footwear
and preventive foot health behaviors
education
Follow-up
- Every 4-6 months
Priority

Indications
- Satisfactory sensitivity
- No ulcers
- Possible foot deformity
- No peripheral artery disease
Timeline
- Referral within 3 months
- Patient needs foot care and preventive
foot health behaviors education
Follow-up
- Once a year
Proper surgical procedure is the responsibility of the medical professional. This information is furnished as an informative guideline. Each surgeon must evaluate the appropriateness of a technique based on his or her personal medical credentials and experience.

The importance of a multidisciplinary approach
Patients with diabetes and Charcot Foot and Ankle represent a special population that may differ in the diagnosis and treatment compared to patients with Charcot Neuroarthropathy due to other reasons. The gold standard for diabetes-related foot complications involves a multidisciplinary healthcare team, where the diabetic foot specialist and the diabetologist play coordinating roles.
In multidisciplinary approaches that are built around the diabetic foot, the timely assessment and diagnosis of wounds, as well as the appropriate methods of prevention and treatment, are the keys to improved evidence-based outcomes:
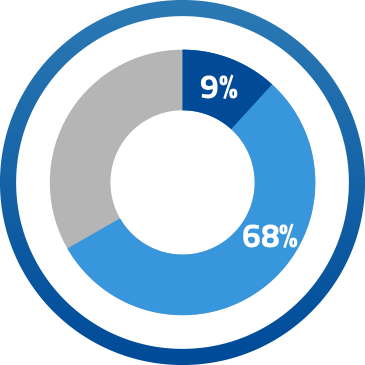
Increased limb salvage,
as a result of a 68% increase
in angioplasty and 9% increase
in bypass operations
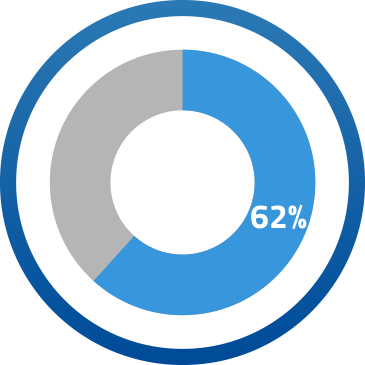
62% reduction
in major amputations
12% reduction in hospitalization
for diabetes-related foot
complications
20% reduction
in overall amputations

The team may also include:
- Vascular surgeons
- Endovascular interventionists/radiologists
- Diabetes nurses
- Pedorthists/orthotists
- Physical therapists

Timely diagnosis of Charcot Foot and Ankle is essential to proper management.
There are four domains involved in the diagnosis of Charcot Foot and Ankle:
- Clinical assessment, including a physical exam and patient history
- Peripheral neuropathy exam
- Initial imaging and laboratory values
- Pedorthists/orthotists
- Charcot Foot and Ankle stage confirmation
The imaging tests play an important role in Charcot Foot diagnosis. Among the imaging techniques
most used are Radiography, Radionuclide, Computerized Tomography, and Magnetic Resonance.

Radiography
The imaging tools, namely radiographs, are fundamental in the diagnostic process in all
stages of the disease.
Radionuclide
The use of nuclear medicine to perform bone scans with small amounts of radioactive tracers
(radionuclides) is valuable to have a functional method of diagnosis, as opposed to the purely
anatomical methods offered by other imaging tools.

Computerized Tomography
Although the use of CT scans in neuropathic arthropathy is not well investigated, this imaging
tool has higher sensitivity for early intra-articular fractures that are not readily visualized in
plain radiographs. CT can also show periosteal new bone formation and small foci of gas
within bone in a better way than MRI can.

Magnetic Resonance
The use of MRI is becoming increasingly popular for the diagnosis of Charcot Foot and Ankle,
especially in the early stage (Eichenholtz Stage 0), which is marked by inflammation. When
applied to the musculoskeletal system, MRI provides excellent soft-tissue contrast resolution
and multiplanar capabilities.

How to prevent Charcot Foot and Ankle
Since the alterations caused by Charcot Foot and Ankle may be initially elusive, it is important that they are detected as soon as possible. To accomplish this, the patient must be aware of his or her crucial role in the disease management by doing regular check-ups, carefully taking care of their feet, and promptly communicating any alteration to a member of their healthcare team.
Failing to take preventative measures and delaying treatment can result in burdensome complications, such as pronounced foot deformity, ulcers, infection, and ultimately lead to limb amputation.





NICE 2017. Diabetic foot problems : prevention and management. Guidance and Guidelines, in https://www.nice.org.uk
Ferreira RC, Goncalez DH et al. 2012. Midfoot Charcot Arthropathy in diabetic Patients: Complication of an epidemic disease in Rev Bras Ortop. Sep-Oct; 47(5):616-25.
Geiss LS, LI Y et al. 2018. Resurgence of diabetes-related nontraumatic lower extremity amputation in the young and middle-aged adult US population; Nov. Diabetes Care in: https://doi.org/10.2337/dc18-1380.
Wukich DK, Amstrong DG et al. 2013. Inpatient Management of Diabetic Foot Disorders: a Clinical Guide. Diabetis Care, Sept; 36(9)2862-71.
American College of Foot and Ankle Surgeons 2017. Clinical Practice Guidelines. www.acfas.org
Australian and International Guidelines on Diabetic Foot Disease 2016. www.diabeticfootaustralia.org
Amit Kumar CJ 2012. A new classification of diabetic foot complications: a simple and effective teaching tool, Journ diabet Foot Complications; 4(1):1.5.
Amstrong DG, Frykberg RG 2003. Classifying diabetic foot surgery: toward a rational definition. Diabet Med. 20(4):329-31.
Andrew J, Rosenbaum MD et al 2015. Classification in brief: Eichenholtz Classification of Charcot Arthropathy. Clin Othop Res 473:1168-71.
Bakker K, Schaper NC 2012, on behalf of the International Working Group on the Diabetic Foot Editorial Board. The development of global consensus guidelines on the management and prevention of the diabetic foot. Diabetes Metab Res Rev; 28(Suppl 1):116-18.
Banskota B, Bijukachhe B et al. 2010. Charcot Neuroarthropathy of the Foot and Ankle. Nepal Orthop Ass J (NOAJ); 1(1):1-6.
Baravarian B, Van Gills CC 2004. Arthrodesis of the Charcot foot and ankle. Clin Podiatr Med Surg; 21(2):271-89.
Bevan WP, Tomlinson MP 2008. Radiographic measures as a predictor of ulcer formation in diabetic Charcot midfoot. Foot Ankle Int. 29(6):568-73.
Bevilacqua NJ 2009. Current Insight on classifying Charcot Arthropathy. Podiatry Today; 22(4):1-5.
Blume PA 2014. Medical and Surgical management of the diabetic foot and ankle. Clin Podiatr Med Surg; 31(1):xiii-xiv.
Blume PA, Sumpio B et al. 2014. Charcot neuroarthropathy of the foot and ankle: diagnosis and management strategies. Clin Podiatr Med Surg 31(1):151-72.
Brodsky JW. The diabetic foot, in Coughlin MJ, Mann RA et al. eds. 2006 Surgery of the Foot and Ankle. St. Louis, MO, USA; Mosby:1281-1368.
Burroughs KE, Reimer CD et al. 1998. Lisfranc Injury of the foot: a commonly missed diagnosis. Am Fam Physician; 58(1):118-24.
Capobianco CM, Ramanujam CL et al. 2010. Charcot foot reconstruction with combined internal and external fixation: case report. J Orthop Surg Res; 5-7.
Caputo GM, Ulbrecht J et al 1998. The Charcot foot in diabetes: six key points. Am Fam Physician; 57(11):2705-10.
Chantelau E, Poll LW 2006. Evaluation of the diabetic Charcot foot by MR imaging or plain radiography – an observational study. Exp Clin Endocrinol Diabetes; 114:428-31.
Chantelau EA, Grützner G 2014. Is the Eichenholtz classification still valid for the diabetic Charcot foot? Swiss Med Wkly; 13:409-14.
Coughlin MJ, Mann RA et al. eds. 2007. Surgery of the foot and ankle; Mosby Elsevier: 1341.
Dalla Paola L. 2014. Confronting a dramatic situation: the Charcot Foot complicated by Osteomyelitis. Int J Low Extrem Wounds; 13(4):247-62.
Dalla Paola L, Brocco E et al. 2009. Limb salvage in Charcot foot and ankle osteomyelitis: combined use single stage/double stage of arthrodesis and external fixation. Foot Anke Int; 30(11):1065-70.
Donegan R, Sumpio B et al. 2013. Charcot foot and ankle with osteomyelitis. Diabet Foot Ankle; 4:10.3402/dfa.v4i0.21361.
Edmonds ME, Foster AVM 2005. Managing the diabetic foot, 2nd ed. Blackwell Science, Oxford UK.
Edmonds ME, Foster AVM, Sanders LJ 2008. A practical Manual of Diabetic Foot care, Blackwell Publishing, USA.
Eichenholtz SN 1966. Charcot Joints. Springfield IL, USA: Charles C. Thomson.
Frykberg RG, Zgonis T et al. 2006 rev. Diabetic Foot disorders: a Clinical Practice Guideline. The Journ of Foot & Ankle Surgery, 45(5):2-66.
Galhoum AE, Abd-Ella MM 2016. Charcot Ankle Neuroarthropathy Pathology, Diagnosis and Management: a Review of Literature, MOJ Orthop Rheumatol; 6(2):00218.
Garapati R, Weinfeld SB 2004. Complex Reconstruction of the diabetic foot and ankle. Am J Surg; 187:81S-86S.
Giurini J 2005. A Closer Look at Fixation Options for the Charcot Foot. Podiatry Today; 18(11).
Grant WP, Garcia-Lavin S et al. 2011. Beaming the columns for Charcot diabetic reconstruction: a retrospective analysis. J Foot Ankle Surg; 50:182-9.
Grant WP, Garcia-Lavin SE et al. 2009. A retrospective analysis of 50 consecutive Charcot diabetic salvage reconstructions. J Foot Ankle Surg; 48(1):30-8.
Grant W, Grant L et al. 2015. Point-counterpoint: is external fixation with Beams better than Internal Fixation?. Podiatry Today; 28(7):1-6.
Grover Pàez F, Totsuka Sutto SE et al. 2013. The diabetic Charcot foot - New insight of treatment, Intech; http://dx.doi.org/10.5772/56399
Güven MF, Karabiber A et al. 2013. Conservative and surgical treatment of the chronic Charcot foot and ankle, Diabet Foot Ankle; 4:10.3402.
Gupta PPK, Mohan V 2003. Charcot foot – un update. Japi; 51:367-72.
Hanft JR, Goggin JP et al. 1998. The role of combined magnetic field bone growth stimulation as an adjunct in the treatment of neuroarthropathy/Charcot joint: an expanded pilot study. J Foot Ankle Surg; 37:510-15, discussion 550-1.
Hastings MK, Johnson JE et al. 2013. Progression of foot deformity in Charcot neuropathic osteoarthropathy. J Bone Joint Surg Am; 95(13):1206-13.
Hastings MK, Sinacore DR et al. 2011.Precision of foot alignment measuyres in Charcot arthropathy. Foot Ankle Int; 32(9):867-72.
Healios Wound Solutions 2017. Management of Charcot Foot. www.healioswoundsolutions.com
Hegewald KW, Wilder ML et al. Combined internal and external fixation for diabetic caharcot reconstruction: a retrospective case series. J Foot Ankle Surg. 55(3):619-27.
Illgner U, Budny T et al. 2014. Clinical benefit and improvement of activity level after reconstruction surgery of Charcot feet using external fixation: 24-months results of 292 feet. BMC Muscoloskeletal Disorders, 15:392.
Ismail I, Dhanapathy A et al. 2015. Diabetic foot complications in a secondary foot hospital:a clinical audit. Australasian Med Jour; 8(4):106-12.
Jeffcoate WJ, Chipcase SY et al. 2006. Assessing the Outcome of the management of Diabetic Foot Ulcers using ulcer-related and person-related measures, Diabetic care; 29(8):1784-87.
Jensen PM, Steinberg JS 2003. Managing Ulcers on the Charcot Foot. Podiatry Today; 16(7):art1774.
Johnson JE 1998. Operative treatment of neuropathic arthropathy of the foot and ankle. J bone Joint Surg; 80_A:1700-09.
Johnson JE, Thomson AB 2008. Charcot Neuroarthopathy of the Foot : Surgical Aspects. Levin and O’ Neal’s The Diabetic Foot; 461-484.
Jones KB, Maiers-Yelden KA et al. 2005. Ankle fractures in patients with diabetes mellitus. J Bone Joint Surg; 87(4): 489-95.
Jude EB, Selby PL et al. 2001. Bisphosphonates in the treatment of Charcot neuroarthropathy: a double-blind randomised control trial. Diabetologia; 44:2032-7.
Koller A, Springfeld R et al. 2011. German-Austrian consensus on operative treatment of Charcot neuroarthropathy: a Perspective by the Charcot task force of the German Association for Foot Surgery, Diabet Foot Ankle, 2:10207.
Lamm BM, Paley D 2007. Charcot neuroarthropathy of the foot and ankle. In: Rozbruch RS, Ilizarov S (eds). Limb lengthening and reconstruction surgery. Informa Healthcare, NY; 16(V):221-32.
Lavery LA, Amstrong DG et al. 1996. Classification of diabetic foot wounds. J Foot Ankle Surg; 35(6):528-31.
Lavery LA, Peters EJG et al. 2010. High Risk Diabetic foot: Treatment and Prevention, CRC Press, NY - London.
Lee L, Blume PA et al. 2003. Charcot joint desease in diabetes mellitus. Ann Vasc Surg;
17(5):571-80.
Lesens O, Desbiez F et al. 2011. Culture of per-wound bone specimens: a simplified approach for the medical management of diabetic foot osteomyelitis. Clin Microbiol Infect, 17(2):285-91.
Liu G 2008. Is External Fixation Overutilized In Managing Charcot In The Diabetic Foot? Podiatry Today; 21(2):1-6.
McEwen LN, Ylitalo KR et al. 2013. Prevalence and risk factors for diabetes related foot complication
in Traslating Research Into action for diabetes (TRIAD). J Diabetes Complications; 27(6): .doi:10.1016/.
Mittlmeier T, Klaue K et al. 2010. Should one consider primary surgical reconstruction in Charcot arthropathy of the feet? Clin Orthop Relat Res; 468:1002-11.
Mrugeshkumar S, Panis W et al. 2016. Charcot Arthropathy treatment and management. Medscape: www.emedicine.medscape.com
Myerson M, Papa J et al. 1992. The total-contact cast for management of neuropathic plantar ulceration of the foot. J Bone Joint Surg; 74-A:261-9.
Petrova NL, Edmonds ME 2016. Acute Charcot neuro-osteoarthropathy. Diabetes Metab Res Rev; 32(1):281-6.
Pinzur MS 2000. Charcot’s foot. Foot Ankle Clin; 5(4):897-912.
Pinzur MS 2006. The role of ring external fixation in Charcot foot arthropathy. Foot ankle Clin. 11(4):837-47.
Pinzur MS 2007. Neutral ring fixation for high-risk nonplantigrade Charcot foot deformity. Foot Ankle Int. 28(9):961-6.
Pinzur MS, Jones C et al. 2017 Instructional Course Lecture # 425 Surgical Treatment of the Charcot Foot, American Academy of Orthopaedic Surgeons (AAOS) Annual Meeting, San Diego CA.
Pinzur MS, Sage R et al. 1993. A treatment algorithm for neuropathic (Charcot) midfoot deformity. Foot Ankle; 14(4):189-97.
Pupp GR, Savage DT et al. 2002. What are the best modalities for Charcot’s Foot? Podiatry Today; 15(12):1042.
Ramanujam CL, Facaros Z et al. 2006. External fixation for surgical off-loading of diabetic
soft tissue reconstruction. Clin Podiatr Med Surg; 23:467-83.
Ramanujam CL, Stapleton JJ et al. 2013. Current concepts with external fixation and the Charcot foot. Podiatry Today; 26(10):1-4.
Ramsey SD, Newton K et al. 1999. Incidence, outcomes and cost of foot ulcers in patients with diabetes. Diabetes Care; 22:382-87.
Richter M, Mittlmeier T. 2015. Intramedullary fixation in severe Charcot osteo-neuroarthropathy with foot deformity results in adequate correction without loss of correction. Results from a multi-centre study. Foot Ankle Sur; 21(2015):269-76.
Robinson AHN, Pasapula C et al. 2009. Surgical aspects of the diabetic foot. J Bone Joint Surg (Br); 91-B:1-7.
Rogers LC, Frykeberg RG et al. 2011. The Charcot Foot in Diabetes. Diabetes Care; 34(9):2123-9.
Rosenbaum AJ, Di Preta JA 2015. Classifications in Brief: Eichenholtz Classification of Charcot Arthropathy. Clain Orthop Relat Res; 473: 1168-1171.
Safavi PS, Jupiter DC et al. 2017. A Systematic Review of Current Surgical Interventions for Charcot Neuroarthropathy of the Midfoot. The J of Foot & Ankle Surg; 56:1249-1256.
Schon LC, Weinfeld SB et al. 1998. Radiographic and Clinical Classification of Acquired Midtarsus Deformities, Foot Ankle Intern; 19(6):394-404.
Short DJ, Zgonis T 2017. Circular External Fixation as a Primari or Adjunctive Therapy for the Podoplastic Approach of the Diabetic Foot. Clin Podiatr Med Surg; 34:93-98.
Shade VL 2015. When should you operate on the Charcot foot? Podiatry Today; 28(3).
Shade VL, Andersen CA 2015. A literature-based guide to the conservative and surgical management of the acute Charcot foot and ankle. Diabet Foot Ankle; 6:10.3402/dfa.v6.26627.
Shahbazian H, Yazdanpanah L et al. 2013. Risk assessment of patients with diabetes for foot ulcers according to risk classification consensus of international working group on diabetic foot. Pak J Med; 29(33):730-34.
Shank CF, Feibel JB 2006. Osteomyelitis in the diabetic foot: diagnosis and management. Foot Ankle Clin; 11(4):775-89.
Shaw JE, Sicree RA et al. 2010. Global estimates of the prevalence of diabetes for 2010 and2030. Diabetes Res Clin Pract; 87(1):4-14.
Shibata T, Tada K et al. 1990. The results of arthrodesis of the ankle for leprotic neuroarthropathy. J Bone Joint Surg Am; 72:749-56.
Shibuya N, Humphers JM et al. 2013. Factors associated with non-union, delayed union and malunion in foot and ankle surgery in diabetic patients, J Foot Ankle Surg; 52(2):207-11.
Short DJ, Zgonis T 2017. Circular External Fixation as a Primary or Adjunctive Therapy for the Podoplastic Approach of the Diabetic Foot. Clin Podiatr Med Surg; 34:93-8.
Simon SR, Tejwani SG et al. 2000. Arthrodesis as an early alternative to non operative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am; 82-A(7): 939-50.
Sinacore DR. Withrington NC 1999. Recognition and management of acute neuropathic (Charcot) Arthropaties of the foot and ankle. J Orthop Sports Phys Ther; 29:736-46.
Sinacore DR. 1998. Acute Charcot arthropathy in patients with diabetes mellitus: healing times by foot location. J Diabetes Complications; 12:287-93.
Sommer TC, Lee TH 2001. Charcot foot: the diagnostic dilemma. Am Fam Physician; 64:1591-98.
Sticha RS, Frascone ST et al. 1996. Major arthrodeses in patients with neuropathic arthropathy, J Foot Ankle Surg; 35(6):560-6.
Trevino SG, De Berardino TM et al. 2011, updated 2016. Lisfranc Fracture Dislocation. Medscape;1236228.
Wang JC 2003. Use of external fixation in the reconstruction of the Charcot foot and ankle. Clin Podiatr Med Surg; 20(1):97-117.
WHO Fact sheet n. 312, updated 2014.
Wu L, Hou Q et al. 2015. Prevalence of risk factors for diabetic foot complications in a Chianese tertiary hospital. Int J Clin Exp Med; 8(3):3785-92.
Yeoh J, Muir KR et al. 2008. Lisfranc fracture-dislocation precipitating acute Charcot arthropathy in a neuropatic diabetic foot: a case report. Cases Jour; 1:290.
Zgonis T, Roukis TS et al. 2007. Charcot foot and ankle reconstruction: current thinking and surgical approaches. Clin Podiatr Med Surg; 24:505-17.
Zgonis T, Jolly GP et al. 2004. External fixation use in arthrodesis of the foot and ankle.
Clin Podiatr Med Surg; 21(1):1-15.