The Surgical Management of Neuropathic
(Charcot) Foot: From Initial Diagnosis
to Surgical Procedures and Beyond
Charcot arthropathy is a complex problem, arising from peripheral neuropathy that is more prevalent among patients with diabetes. Surgical reconstruction is a challenging procedure associated with a high complication rate. Despite its complexity, foot reconstruction is indicated in cases of advanced disease, with the goal being to salvage the patient’s limb and improve their quality of life.
Timely diagnosis and appropriate treatment are essential to prevent joint instability and bone destruction and, in extreme cases, limb amputation.
Are you a patient? Go to LimbHealing.com

What is the essential
literature about
Charcot arthropathy?

How do experts
define Charcot
arthropathy?

What are the initial
symptoms and how is
Charcot arthropathy
diagnosed?

What are the various
surgical approaches
when performing
Charcot foot
reconstruction?

Which surgical
procedures and
fixation methods are
available for Charcot
arthropathy?

What is the optimal
postoperative
treatment after foot
reconstruction?

What Is the Essential Literature
About Charcot Arthropathy?
There are many scientific articles about Charcot foot, and it may be difficult to sift through the existing literature.
Still, it is possible to have a collection of essential reviews, books, and articles pertaining to this pathology.
For an overview of all aspects of Charcot arthropathy, clinicians are advised to read:
- “The Charcot Foot in Diabetes,” a summary of the available evidence on the pathophysiology, natural history, presentations, and treatment recommendations. This publication was authored by of an international task force of experts who were brought together by the American Diabetes Association and the American Podiatric Medical Association.
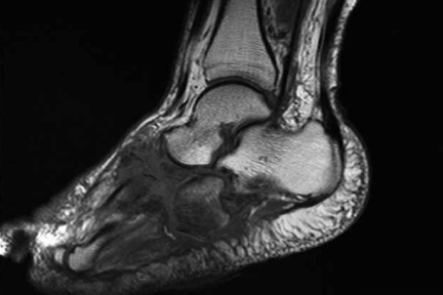
- “The Essentials of Charcot Neuroarthropathy,” edited by Claude Pierre-Jerome, covers the epidemiology, biomechanics, pathophysiology, socioeconomic impacts, radiological findings, and differential diagnosis of Charcot foot in diabetic patients, with an emphasis on MRI.
For articles on the treatment, we suggest:
- “Nonoperative Treatment of Charcot Neuro-osteoarthropathy,” by Felix W.A. Waibel and Thomas Böni, which has a specific focus on conservative management but also advises when surgical treatment should be considered.
- “Surgical Considerations for the Acute and Chronic Charcot Neuroarthropathy of the Foot and Ankle,” by Alan C. Stuto and John J. Stapleton. In this article, the authors explain how surgical procedures are chosen based on the clinical scenario and the specific goals of the surgery.
There are several articles on fixation devices for Charcot foot reconstruction, including:
- “Charcot foot reconstruction outcomes: A systematic review,” where the authors report on a total of 1116 feet in 1089 patients, who were managed with external or internal fixation, or with a combination of both.
- “Beaming the Charcot Foot,” by Drs. William Grant and Lisa Grant-McDonald. In this article, the authors address the mechanics, technique, and hardware considerations of ‘superconstructs,’ a method where some of the normal principles of orthopedic techniques are abandoned to improve stability and reduce the likelihood of failure.
There is an ever-expanding number of articles about Charcot arthropathy, and we will be updating our collection regularly to provide you with the most current information.

How Do Experts Define
Charcot Arthropathy?
According to an international task force of experts, Charcot arthropathy can be described as:
“A condition affecting the bones, joints,
and soft tissues of the foot and ankle,
characterized by inflammation in the
earliest phase.”
In later stages, the interaction of metabolic, neuropathic, and traumatic factors “may lead to varying degrees
and patterns of bone destruction, subluxation, dislocation, and deformity.”
Although it was first diagnosed more than 130 years ago, Charcot arthropathy in the diabetic patient remains
a challenge for clinicians to treat. Due to its rareness, a general practitioner may only encounter a Charcot case every 13 years.
The natural progression of diabetic Charcot foot typically follows three stages, as described by Eichenholtz in 1966:

Stage I
Acute or
fragmentation phase

Stage II
Subacute or
coalescence phase

Stage III
Consolidation and
reconstructive phase
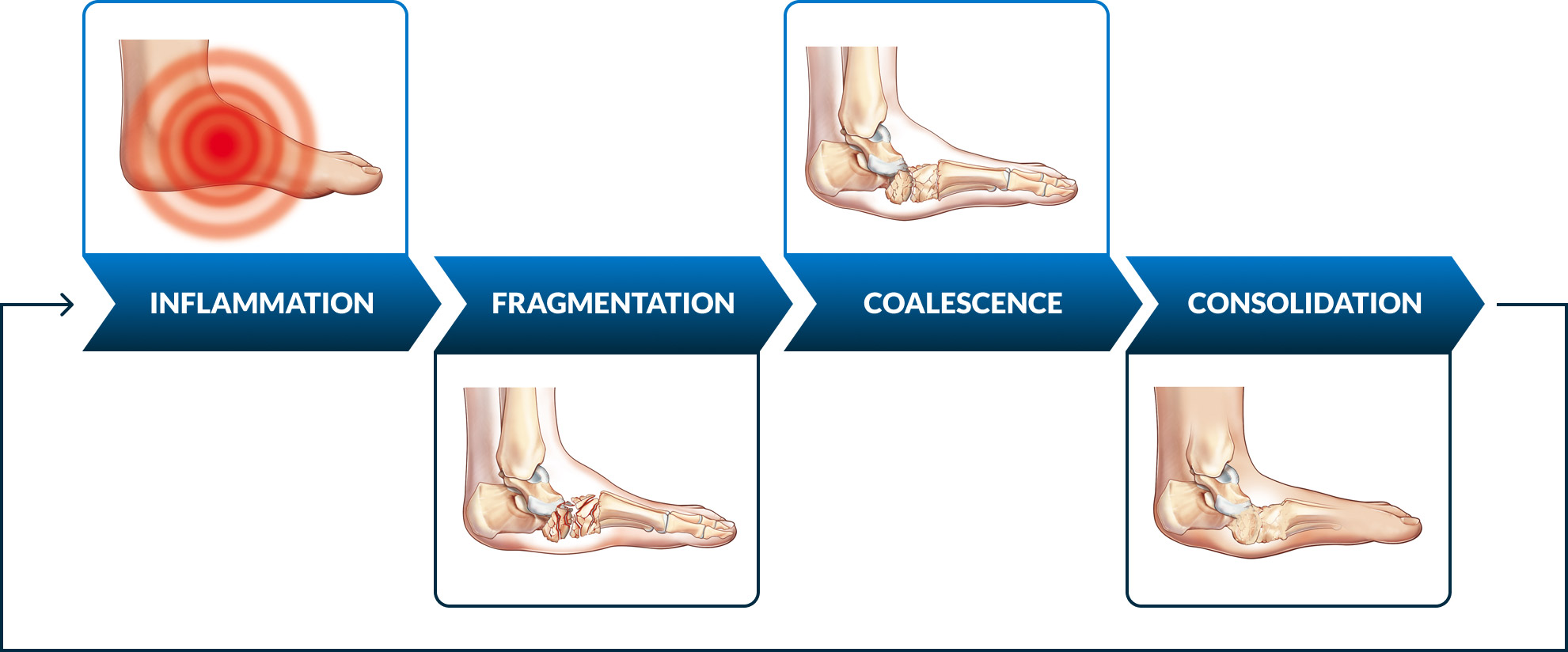
Each one of these stages is accompanied by radiographic findings. Later, the modified Eichenholtz classification introduced an additional stage named prodromal or stage 0, to reflect the clinical findings related to inflammation that are not yet visible on radiographs.
Other authors propose classification systems that focus on the anatomical aspects of neuropathic arthropathy, highlighting the involved joints in each case.
The consequences of untreated Charcot arthropathy can be devastating for patients, so a timely diagnosis is paramount. An attentive clinician can distinguish between a Charcot case and other pathologies and improve their patient’s outcomes.

What Are the Initial Symptoms and How Is Charcot Arthropathy Diagnosed?
According to the modified Eichenholtz classification, the natural history of the pathology involves four different stages, often grouped in active versus non-active disease states: inflammation, fragmentation, coalescence, and consolidation. Patients usually only go through one round of the different stages, but approximately 23% of them can suffer through multiple cycles, resulting in high morbidity and severe foot deformity.
There is not a single diagnostic test to clearly diagnose Charcot arthropathy, and the best safeguard for clinicians to avoid missing a case is to always be suspicious. According to the experts, these are the clinical signs that can be found in a patient with Charcot arthropathy:
- A warm, swollen, and sometimes erythematosus and red foot. These signs indicate inflammation, which is present in acute Charcot foot.
- Concomitant ulceration or crepitus during examination, with patients often reporting a series of minor trauma.
- Absence of pain, due to peripheral neuropathy.
In addition to the clinical assessment, the following imaging techniques are recommended:



A rapid and accurate Charcot diagnosis is essential to protect the foot and reduce the chance of further bony collapse of the foot and ankle. Patients benefit from attentive physicians well versed in its treatment and a multidisciplinary approach where all specialists work together.
When is time for a specialist?
Priority
Indications
Timeline
Follow-up
Priority

Indications
- Open wounds and deep ulcers
- Pain at rest
- Active Charcot Foot deformity
(red, hot, swollen) - Vascular compromise
Timeline
- Urgent/immediate referral
- Patient needs interdisciplinary care
management, off-loading with total
contact cast devices and/or surgery,
diabetic orthopedic footwear
Follow-up
- According to specialist decision
Priority

Indications
- No sensitivity
- Ulcers
- Chronic vascular venous insufficiency
- Previous lower limb amputation
related to diabetes
Timeline
- Immediate/first available referral
- Patient needs diabetic orthopedic
footwear, preventative off-loading
and appropriate therapy
Follow-up
- Every 1-2 months
Priority

Indications
- Insufficient sensitivity
- No ulcers
- Foot deformity
- Posterior tibial pulse diminished
or absent - Foot swelling, aedema
Timeline
- No ulcers
- Foot deformity
- Posterior tibial pulse diminished
- or absent
- Foot swelling, edema
- Referral within 3 weeks
- Patient needs prescriptive footwear,
preventative off-loading and
appropriate therapy
Follow-up
- Every 2-3 months
Priority

Indications
- Insufficient sensitivity
- No ulcers
- No foot deformity
Timeline
- Referral within 1 months
- Patient needs prescriptive footwear
and preventive foot health behaviors
education
Follow-up
- Every 4-6 months
Priority

Indications
- Satisfactory sensitivity
- No ulcers
- Possible foot deformity
- No peripheral artery disease
Timeline
- Referral within 3 months
- Patient needs foot care and preventive
foot health behaviors education
Follow-up
- Once a year
Proper surgical procedure is the responsibility of the medical professional. This information is furnished as an informative guideline. Each surgeon must evaluate the appropriateness of a technique based on his or her personal medical credentials and experience.


What are the various surgical approaches when performing Charcot foot reconstruction?
Regardless of the chosen approach, the goals of Charcot arthropathy treatment are to achieve a stable plantigrade foot resistant to ulceration, prevent amputation, and improve the patient's quality of life.
When conservative management is not enough to achieve these goals, surgical reconstruction should be considered, and preferably performed during the non-active disease state.
Although ideally every collapsed or deformed Charcot arthropathy case would be surgically transformed into a stable and ambulatory foot, unfortunately not all patients can undergo major reconstructive surgery. Other (non-reconstructive) surgery options include:

Muscle flaps, which may
be used to provide soft
tissue coverage

Equinus correction

Correction of residual varus
deformities
The most common methods of Charcot foot fixation are internal fixation, external fixation, or a combination of both. Selecting the right surgical technique for Charcot arthropathy fixation is challenging, and surgery requires careful planning.

What Surgical Procedures and Fixation Methods
Are Available for Charcot Arthropathy?
In the past, surgical reconstruction to address Charcot arthropathy was considered a limb salvage procedure, used as a last resort to avoid amputation. Currently, there has been a shift in the way of thinking, and surgeons also perform these same reconstructive procedures so that their patients can use commercially available footwear instead of orthoses, thus improving their quality of life.
Charcot foot reconstruction can be achieved with internal fixation, external fixation, or a combination of both internal and external fixation, also called hybrid fixation. Patients with Charcot arthropathy require a highly individualized treatment approach, and the choice of treatment will depend on several factors:
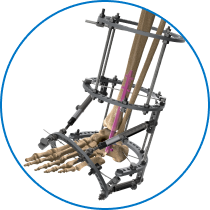
Internal fixation is often used in midfoot pathologies, commonly employing beams or plates.
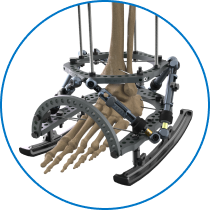
External fixation is recommended in the presence of poor-quality bone, compromised soft tissue, active infection, or osteomyelitis. In such cases, internal fixation is not recommended. External fixation has the additional benefit of allowing early weightbearing.
Hybrid constructs can be particularly useful in the treatment of Charcot arthropathy of the ankle, where secure fixation is essential to maintain biomechanics and proprioception.
Recently new techniques have emerged, including the use of superconstructs, which maximize stability by extending the use of hardware beyond the zone of injury. This technique uses two or more devices, such as a medial column plate positioned over a beam, which are positioned in a way that optimizes mechanical integrity. By using superconstructs, some of the problems caused by poor-quality bone can be avoided by using non-affected bone
for fixation.
Surgical reconstruction of a Charcot foot is technically demanding, with added challenges posed by the presence
of diabetes, neuropathy, poor bone quality, and possibly infection. Despite these obstacles, it is possible to obtain successful clinical outcomes with thorough preoperative planning and the collaboration of a multidisciplinary team.

What Is the Optimal Postoperative
Treatment After Foot Reconstruction?
To improve the odds of a successful treatment, postoperative care should be a priority in patients with Charcot arthropathy. This is especially true in extensive reconstructive surgeries, for which rehabilitation and postoperative management require extensive resources and patient compliance.
Since Charcot patients have peripheral neuropathy and often also have diabetes, they have a higher risk of complications following surgery, including:
- Pin site infection when external fixation is used
- Deep infection
- Hardware failure
- Unstable non-union
- Wound dehiscence
- Metabolic perturbations, which can change normal glucose homeostasis.
For patients treated with internal fixation, there is a more prolonged period in which weight-bearing is not possible. It is essential to make sure that patients have an adequate support, so they adhere to the non-weightbearing limitation.
Although surgeons might be tempted to overly focus on the operative technical aspects or the best device(s) for each individual case, it is also important to pay close attention to the postoperative treatment, which is critical in ensuring successful surgical outcomes.
Learn more about the surgical management of Charcot
Arthropathy with our Surgical Case Reports
Choosing the right surgical approach and post-operative treatment for a Charcot foot is unquestionably
a challenge for the orthopedic specialist. To know more about how our experts have surgically treated
their patients, we have compiled a series of Charcot Foot Reconstruction Case Reports.





Timely diagnosis and appropriate treatment are essential to prevent joint instability and bone destruction and,
in extreme cases, limb amputation. If you want to learn more about how to prevent Charcot Foot and Ankle,
please look at “Charcot Neuropathy in the Diabetic Foot: Incidence, Causes, Symptoms and Diagnosis” page.
NICE 2017. Diabetic foot problems : prevention and management. Guidance and Guidelines, in https://www.nice.org.uk
Ferreira RC, Goncalez DH et al. 2012. Midfoot Charcot Arthropathy in diabetic Patients: Complication of an epidemic disease in Rev Bras Ortop. Sep-Oct; 47(5):616-25.
Geiss LS, LI Y et al. 2018. Resurgence of diabetes-related nontraumatic lower extremity amputation in the young and middle-aged adult US population; Nov. Diabetes Care in: https://doi.org/10.2337/dc18-1380.
Wukich DK, Amstrong DG et al. 2013. Inpatient Management of Diabetic Foot Disorders: a Clinical Guide. Diabetis Care, Sept; 36(9)2862-71.
American College of Foot and Ankle Surgeons 2017. Clinical Practice Guidelines. www.acfas.org
Australian and International Guidelines on Diabetic Foot Disease 2016. www.diabeticfootaustralia.org
Amit Kumar CJ 2012. A new classification of diabetic foot complications: a simple and effective teaching tool, Journ diabet Foot Complications; 4(1):1.5.
Amstrong DG, Frykberg RG 2003. Classifying diabetic foot surgery: toward a rational definition. Diabet Med. 20(4):329-31.
Andrew J, Rosenbaum MD et al 2015. Classification in brief: Eichenholtz Classification of Charcot Arthropathy. Clin Othop Res 473:1168-71.
Bakker K, Schaper NC 2012, on behalf of the International Working Group on the Diabetic Foot Editorial Board. The development of global consensus guidelines on the management and prevention of the diabetic foot. Diabetes Metab Res Rev; 28(Suppl 1):116-18.
Banskota B, Bijukachhe B et al. 2010. Charcot Neuroarthropathy of the Foot and Ankle. Nepal Orthop Ass J (NOAJ); 1(1):1-6.
Baravarian B, Van Gills CC 2004. Arthrodesis of the Charcot foot and ankle. Clin Podiatr Med Surg; 21(2):271-89.
Bevan WP, Tomlinson MP 2008. Radiographic measures as a predictor of ulcer formation in diabetic Charcot midfoot. Foot Ankle Int. 29(6):568-73.
Bevilacqua NJ 2009. Current Insight on classifying Charcot Arthropathy. Podiatry Today; 22(4):1-5.
Blume PA 2014. Medical and Surgical management of the diabetic foot and ankle. Clin Podiatr Med Surg; 31(1):xiii-xiv.
Blume PA, Sumpio B et al. 2014. Charcot neuroarthropathy of the foot and ankle: diagnosis and management strategies. Clin Podiatr Med Surg 31(1):151-72.
Brodsky JW. The diabetic foot, in Coughlin MJ, Mann RA et al. eds. 2006 Surgery of the Foot and Ankle. St. Louis, MO, USA; Mosby:1281-1368.
Burroughs KE, Reimer CD et al. 1998. Lisfranc Injury of the foot: a commonly missed diagnosis. Am Fam Physician; 58(1):118-24.
Capobianco CM, Ramanujam CL et al. 2010. Charcot foot reconstruction with combined internal and external fixation: case report. J Orthop Surg Res; 5-7.
Caputo GM, Ulbrecht J et al 1998. The Charcot foot in diabetes: six key points. Am Fam Physician; 57(11):2705-10.
Chantelau E, Poll LW 2006. Evaluation of the diabetic Charcot foot by MR imaging or plain radiography – an observational study. Exp Clin Endocrinol Diabetes; 114:428-31.
Chantelau EA, Grützner G 2014. Is the Eichenholtz classification still valid for the diabetic Charcot foot? Swiss Med Wkly; 13:409-14.
Coughlin MJ, Mann RA et al. eds. 2007. Surgery of the foot and ankle; Mosby Elsevier: 1341.
Dalla Paola L. 2014. Confronting a dramatic situation: the Charcot Foot complicated by Osteomyelitis. Int J Low Extrem Wounds; 13(4):247-62.
Dalla Paola L, Brocco E et al. 2009. Limb salvage in Charcot foot and ankle osteomyelitis: combined use single stage/double stage of arthrodesis and external fixation. Foot Anke Int; 30(11):1065-70.
Donegan R, Sumpio B et al. 2013. Charcot foot and ankle with osteomyelitis. Diabet Foot Ankle; 4:10.3402/dfa.v4i0.21361.
Edmonds ME, Foster AVM 2005. Managing the diabetic foot, 2nd ed. Blackwell Science, Oxford UK.
Edmonds ME, Foster AVM, Sanders LJ 2008. A practical Manual of Diabetic Foot care, Blackwell Publishing, USA.
Eichenholtz SN 1966. Charcot Joints. Springfield IL, USA: Charles C. Thomson.
Frykberg RG, Zgonis T et al. 2006 rev. Diabetic Foot disorders: a Clinical Practice Guideline. The Journ of Foot & Ankle Surgery, 45(5):2-66.
Galhoum AE, Abd-Ella MM 2016. Charcot Ankle Neuroarthropathy Pathology, Diagnosis and Management: a Review of Literature, MOJ Orthop Rheumatol; 6(2):00218.
Garapati R, Weinfeld SB 2004. Complex Reconstruction of the diabetic foot and ankle. Am J Surg; 187:81S-86S.
Giurini J 2005. A Closer Look at Fixation Options for the Charcot Foot. Podiatry Today; 18(11).
Grant WP, Garcia-Lavin S et al. 2011. Beaming the columns for Charcot diabetic reconstruction: a retrospective analysis. J Foot Ankle Surg; 50:182-9.
Grant WP, Garcia-Lavin SE et al. 2009. A retrospective analysis of 50 consecutive Charcot diabetic salvage reconstructions. J Foot Ankle Surg; 48(1):30-8.
Grant W, Grant L et al. 2015. Point-counterpoint: is external fixation with Beams better than Internal Fixation?. Podiatry Today; 28(7):1-6.
Grover Pàez F, Totsuka Sutto SE et al. 2013. The diabetic Charcot foot - New insight of treatment, Intech; http://dx.doi.org/10.5772/56399
Güven MF, Karabiber A et al. 2013. Conservative and surgical treatment of the chronic Charcot foot and ankle, Diabet Foot Ankle; 4:10.3402.
Gupta PPK, Mohan V 2003. Charcot foot – un update. Japi; 51:367-72.
Hanft JR, Goggin JP et al. 1998. The role of combined magnetic field bone growth stimulation as an adjunct in the treatment of neuroarthropathy/Charcot joint: an expanded pilot study. J Foot Ankle Surg; 37:510-15, discussion 550-1.
Hastings MK, Johnson JE et al. 2013. Progression of foot deformity in Charcot neuropathic osteoarthropathy. J Bone Joint Surg Am; 95(13):1206-13.
Hastings MK, Sinacore DR et al. 2011.Precision of foot alignment measuyres in Charcot arthropathy. Foot Ankle Int; 32(9):867-72.
Healios Wound Solutions 2017. Management of Charcot Foot. www.healioswoundsolutions.com
Hegewald KW, Wilder ML et al. Combined internal and external fixation for diabetic caharcot reconstruction: a retrospective case series. J Foot Ankle Surg. 55(3):619-27.
Illgner U, Budny T et al. 2014. Clinical benefit and improvement of activity level after reconstruction surgery of Charcot feet using external fixation: 24-months results of 292 feet. BMC Muscoloskeletal Disorders, 15:392.
Ismail I, Dhanapathy A et al. 2015. Diabetic foot complications in a secondary foot hospital:a clinical audit. Australasian Med Jour; 8(4):106-12.
Jeffcoate WJ, Chipcase SY et al. 2006. Assessing the Outcome of the management of Diabetic Foot Ulcers using ulcer-related and person-related measures, Diabetic care; 29(8):1784-87.
Jensen PM, Steinberg JS 2003. Managing Ulcers on the Charcot Foot. Podiatry Today; 16(7):art1774.
Johnson JE 1998. Operative treatment of neuropathic arthropathy of the foot and ankle. J bone Joint Surg; 80_A:1700-09.
Johnson JE, Thomson AB 2008. Charcot Neuroarthopathy of the Foot : Surgical Aspects. Levin and O’ Neal’s The Diabetic Foot; 461-484.
Jones KB, Maiers-Yelden KA et al. 2005. Ankle fractures in patients with diabetes mellitus. J Bone Joint Surg; 87(4): 489-95.
Jude EB, Selby PL et al. 2001. Bisphosphonates in the treatment of Charcot neuroarthropathy: a double-blind randomised control trial. Diabetologia; 44:2032-7.
Koller A, Springfeld R et al. 2011. German-Austrian consensus on operative treatment of Charcot neuroarthropathy: a Perspective by the Charcot task force of the German Association for Foot Surgery, Diabet Foot Ankle, 2:10207.
Lamm BM, Paley D 2007. Charcot neuroarthropathy of the foot and ankle. In: Rozbruch RS, Ilizarov S (eds). Limb lengthening and reconstruction surgery. Informa Healthcare, NY; 16(V):221-32.
Lavery LA, Amstrong DG et al. 1996. Classification of diabetic foot wounds. J Foot Ankle Surg; 35(6):528-31.
Lavery LA, Peters EJG et al. 2010. High Risk Diabetic foot: Treatment and Prevention, CRC Press, NY - London.
Lee L, Blume PA et al. 2003. Charcot joint desease in diabetes mellitus. Ann Vasc Surg;
17(5):571-80.
Lesens O, Desbiez F et al. 2011. Culture of per-wound bone specimens: a simplified approach for the medical management of diabetic foot osteomyelitis. Clin Microbiol Infect, 17(2):285-91.
Liu G 2008. Is External Fixation Overutilized In Managing Charcot In The Diabetic Foot? Podiatry Today; 21(2):1-6.
McEwen LN, Ylitalo KR et al. 2013. Prevalence and risk factors for diabetes related foot complication
in Traslating Research Into action for diabetes (TRIAD). J Diabetes Complications; 27(6): .doi:10.1016/.
Mittlmeier T, Klaue K et al. 2010. Should one consider primary surgical reconstruction in Charcot arthropathy of the feet? Clin Orthop Relat Res; 468:1002-11.
Mrugeshkumar S, Panis W et al. 2016. Charcot Arthropathy treatment and management. Medscape: www.emedicine.medscape.com
Myerson M, Papa J et al. 1992. The total-contact cast for management of neuropathic plantar ulceration of the foot. J Bone Joint Surg; 74-A:261-9.
Petrova NL, Edmonds ME 2016. Acute Charcot neuro-osteoarthropathy. Diabetes Metab Res Rev; 32(1):281-6.
Pinzur MS 2000. Charcot’s foot. Foot Ankle Clin; 5(4):897-912.
Pinzur MS 2006. The role of ring external fixation in Charcot foot arthropathy. Foot ankle Clin. 11(4):837-47.
Pinzur MS 2007. Neutral ring fixation for high-risk nonplantigrade Charcot foot deformity. Foot Ankle Int. 28(9):961-6.
Pinzur MS, Jones C et al. 2017 Instructional Course Lecture # 425 Surgical Treatment of the Charcot Foot, American Academy of Orthopaedic Surgeons (AAOS) Annual Meeting, San Diego CA.
Pinzur MS, Sage R et al. 1993. A treatment algorithm for neuropathic (Charcot) midfoot deformity. Foot Ankle; 14(4):189-97.
Pupp GR, Savage DT et al. 2002. What are the best modalities for Charcot’s Foot? Podiatry Today; 15(12):1042.
Ramanujam CL, Facaros Z et al. 2006. External fixation for surgical off-loading of diabetic
soft tissue reconstruction. Clin Podiatr Med Surg; 23:467-83.
Ramanujam CL, Stapleton JJ et al. 2013. Current concepts with external fixation and the Charcot foot. Podiatry Today; 26(10):1-4.
Ramsey SD, Newton K et al. 1999. Incidence, outcomes and cost of foot ulcers in patients with diabetes. Diabetes Care; 22:382-87.
Richter M, Mittlmeier T. 2015. Intramedullary fixation in severe Charcot osteo-neuroarthropathy with foot deformity results in adequate correction without loss of correction. Results from a multi-centre study. Foot Ankle Sur; 21(2015):269-76.
Robinson AHN, Pasapula C et al. 2009. Surgical aspects of the diabetic foot. J Bone Joint Surg (Br); 91-B:1-7.
Rogers LC, Frykeberg RG et al. 2011. The Charcot Foot in Diabetes. Diabetes Care; 34(9):2123-9.
Rosenbaum AJ, Di Preta JA 2015. Classifications in Brief: Eichenholtz Classification of Charcot Arthropathy. Clain Orthop Relat Res; 473: 1168-1171.
Safavi PS, Jupiter DC et al. 2017. A Systematic Review of Current Surgical Interventions for Charcot Neuroarthropathy of the Midfoot. The J of Foot & Ankle Surg; 56:1249-1256.
Schon LC, Weinfeld SB et al. 1998. Radiographic and Clinical Classification of Acquired Midtarsus Deformities, Foot Ankle Intern; 19(6):394-404.
Short DJ, Zgonis T 2017. Circular External Fixation as a Primari or Adjunctive Therapy for the Podoplastic Approach of the Diabetic Foot. Clin Podiatr Med Surg; 34:93-98.
Shade VL 2015. When should you operate on the Charcot foot? Podiatry Today; 28(3).
Shade VL, Andersen CA 2015. A literature-based guide to the conservative and surgical management of the acute Charcot foot and ankle. Diabet Foot Ankle; 6:10.3402/dfa.v6.26627.
Shahbazian H, Yazdanpanah L et al. 2013. Risk assessment of patients with diabetes for foot ulcers according to risk classification consensus of international working group on diabetic foot. Pak J Med; 29(33):730-34.
Shank CF, Feibel JB 2006. Osteomyelitis in the diabetic foot: diagnosis and management. Foot Ankle Clin; 11(4):775-89.
Shaw JE, Sicree RA et al. 2010. Global estimates of the prevalence of diabetes for 2010 and2030. Diabetes Res Clin Pract; 87(1):4-14.
Shibata T, Tada K et al. 1990. The results of arthrodesis of the ankle for leprotic neuroarthropathy. J Bone Joint Surg Am; 72:749-56.
Shibuya N, Humphers JM et al. 2013. Factors associated with non-union, delayed union and malunion in foot and ankle surgery in diabetic patients, J Foot Ankle Surg; 52(2):207-11.
Short DJ, Zgonis T 2017. Circular External Fixation as a Primary or Adjunctive Therapy for the Podoplastic Approach of the Diabetic Foot. Clin Podiatr Med Surg; 34:93-8.
Simon SR, Tejwani SG et al. 2000. Arthrodesis as an early alternative to non operative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am; 82-A(7): 939-50.
Sinacore DR. Withrington NC 1999. Recognition and management of acute neuropathic (Charcot) Arthropaties of the foot and ankle. J Orthop Sports Phys Ther; 29:736-46.
Sinacore DR. 1998. Acute Charcot arthropathy in patients with diabetes mellitus: healing times by foot location. J Diabetes Complications; 12:287-93.
Sommer TC, Lee TH 2001. Charcot foot: the diagnostic dilemma. Am Fam Physician; 64:1591-98.
Sticha RS, Frascone ST et al. 1996. Major arthrodeses in patients with neuropathic arthropathy, J Foot Ankle Surg; 35(6):560-6.
Trevino SG, De Berardino TM et al. 2011, updated 2016. Lisfranc Fracture Dislocation. Medscape;1236228.
Wang JC 2003. Use of external fixation in the reconstruction of the Charcot foot and ankle. Clin Podiatr Med Surg; 20(1):97-117.
WHO Fact sheet n. 312, updated 2014.
Wu L, Hou Q et al. 2015. Prevalence of risk factors for diabetic foot complications in a Chianese tertiary hospital. Int J Clin Exp Med; 8(3):3785-92.
Yeoh J, Muir KR et al. 2008. Lisfranc fracture-dislocation precipitating acute Charcot arthropathy in a neuropatic diabetic foot: a case report. Cases Jour; 1:290.
Zgonis T, Roukis TS et al. 2007. Charcot foot and ankle reconstruction: current thinking and surgical approaches. Clin Podiatr Med Surg; 24:505-17.
Zgonis T, Jolly GP et al. 2004. External fixation use in arthrodesis of the foot and ankle.
Clin Podiatr Med Surg; 21(1):1-15.
Abyar, E., McKissack, H., & Johnson, M. D. (2022). Chapter 19 - The surgical management of the Charcot foot: physical examination of the foot prior to surgery, indications and criteria for amputation, and surgical techniques. In C. Pierre-Jerome (Ed.), The Essentials of Charcot Neuroarthropathy (pp. 441-448). Elsevier. https://doi.org/https://doi.org/10.1016/B978-0-323-99352-4.00013-9
Alrashidi, Y., Hügle, T., Wiewiorski, M., Herrera-Perez, M., & Valderrabano, V. (2017). Surgical Treatment Options for the Diabetic Charcot Midfoot Deformity. Clin Podiatr Med Surg, 34(1), 43-51. https://doi.org/10.1016/j.cpm.2016.07.006
Bajuri, M. Y., Ong, S. L., Das, S., & Mohamed, I. N. (2022). Charcot Neuroarthropathy: Current Surgical Management and Update. A Systematic Review. Front Surg, 9, 820826. https://doi.org/10.3389/fsurg.2022.820826
Brandão, R. A., Weber, J. S., Larson, D., Prissel, M. A., Bull, P. E., Berlet, G. C., & Hyer, C. F. (2018). New Fixation Methods for the Treatment of the Diabetic Foot: Beaming, External Fixation, and Beyond. Clin Podiatr Med Surg, 35(1), 63-76. https://doi.org/10.1016/j.cpm.2017.08.001
Brodsky, J. W., & Rouse, A. M. (1993). Exostectomy for symptomatic bony prominences in diabetic Charcot feet. Clin Orthop Relat Res(296), 21-26.
Chen, S., Miller, J. D., & Steinberg, J. S. (2022). Management of the Charcot Foot and Ankle: Nonreconstructive Surgery. Clinics in Podiatric Medicine and Surgery, 39(4), 559-570. https://doi.org/https://doi.org/10.1016/j.cpm.2022.05.003
Dardari, D. (2020). An overview of Charcot's neuroarthropathy. J Clin Transl Endocrinol, 22, 100239. https://doi.org/10.1016/j.jcte.2020.100239
Frykberg, R. G., & Belczyk, R. (2008). Epidemiology of the Charcot Foot. Clinics in Podiatric Medicine and Surgery, 25(1), 17-28. https://doi.org/https://doi.org/10.1016/j.cpm.2007.10.001
Grant, W., & Grant-McDonald, L. (2022). Beaming the Charcot Foot. Clinics in Podiatric Medicine and Surgery, 39(4), 605-627. https://doi.org/https://doi.org/10.1016/j.cpm.2022.05.007
Ha, J., Hester, T., Foley, R., Reichert, I. L. H., Vas, P. R. J., Ahluwalia, R., & Kavarthapu, V. (2020). Charcot foot reconstruction outcomes: A systematic review. J Clin Orthop Trauma, 11(3), 357-368. https://doi.org/10.1016/j.jcot.2020.03.025
Marmolejo, V. S., Arnold, J. F., Ponticello, M., & Anderson, C. A. (2018). Charcot Foot: Clinical Clues, Diagnostic Strategies, and Treatment Principles. Am Fam Physician, 97(9), 594-599.
Martin, B., & Chow, J. (2021). The use of circular frame external fixation in the treatment of ankle/hindfoot Charcot Neuroarthropathy. J Clin Orthop Trauma, 16, 269-276. https://doi.org/10.1016/j.jcot.2021.02.016
Pierre-Jerome, C. (2022). The essentials of Charcot neuroarthropathy: biomechanics, pathophysiology, and MRI findings. Elsevier.
Pinzur, M. S., & Schiff, A. P. (2018). Deformity and Clinical Outcomes Following Operative Correction of Charcot Foot: A New Classification with Implications for Treatment. Foot Ankle Int, 39(3), 265-270. https://doi.org/10.1177/1071100717742371
Rogers, L. C., Frykberg, R. G., Armstrong, D. G., Boulton, A. J. M., Edmonds, M., Van, G. H., Hartemann, A., Game, F., Jeffcoate, W., Jirkovska, A., Jude, E., Morbach, S., Morrison, W. B., Pinzur, M., Pitocco, D., Sanders, L., Wukich, D. K., & Uccioli, L. (2011). The Charcot Foot in Diabetes. Journal of the American Podiatric Medical Association, 101(5), 437-446. https://doi.org/10.7547/1010437
Rosenbaum, A. J., & DiPreta, J. A. (2015). Classifications in brief: Eichenholtz classification of Charcot arthropathy. Clin Orthop Relat Res, 473(3), 1168-1171. https://doi.org/10.1007/s11999-014-4059-y
Rosskopf, A. B., Loupatatzis, C., Pfirrmann, C. W. A., Böni, T., & Berli, M. C. (2019). The Charcot foot: a pictorial review. Insights Imaging, 10(1), 77. https://doi.org/10.1186/s13244-019-0768-9
Salvaterra, P. (2017). The Surgical Management of Neuropathic (Charcot) Foot - A Practical Guideline.
Sammarco, V. J. (2009). Superconstructs in the Treatment of Charcot Foot Deformity: Plantar Plating, Locked Plating, and Axial Screw Fixation. Foot and Ankle Clinics, 14(3), 393-407. https://doi.org/https://doi.org/10.1016/j.fcl.2009.04.004
Sanders, L. (1991). Diabetic neuropathic osteoarthropathy: the Charcot foot. The high risk foot in diabetes mellitus.
Schade, V. L., & Andersen, C. A. (2015). A literature-based guide to the conservative and surgical management of the acute Charcot foot and ankle. Diabet Foot Ankle, 6, 26627. https://doi.org/10.3402/dfa.v6.26627
Schmidt, B. M. (2020). Clinical insights into Charcot foot. Best Pract Res Clin Rheumatol, 34(3), 101563. https://doi.org/10.1016/j.berh.2020.101563
Stuto, A. C., & Stapleton, J. J. (2022). Surgical Considerations for the Acute and Chronic Charcot Neuroarthropathy of the Foot and Ankle. Clinics in Podiatric Medicine and Surgery, 39(2), 331-341. https://doi.org/https://doi.org/10.1016/j.cpm.2021.11.005
Sudhakaran, S., & Surani, S. R. (2015). Guidelines for Perioperative Management of the Diabetic Patient. Surgery Research and Practice, 2015, 284063. https://doi.org/10.1155/2015/284063
Svendsen, O. L., Rabe, O. C., Winther-Jensen, M., & Allin, K. H. (2021). How Common Is the Rare Charcot Foot in Patients with Diabetes? Diabetes Care, 44(4), e62-e63. https://doi.org/10.2337/dc20-2590
Trepman, E., Nihal, A., & Pinzur, M. S. (2005). Current Topics Review: Charcot Neuroarthropathy of the Foot and Ankle. Foot & Ankle International, 26(1), 46-63. https://doi.org/10.1177/107110070502600109
Trieb, K. (2016). The Charcot foot. The Bone & Joint Journal, 98-B(9), 1155-1159. https://doi.org/10.1302/0301-620x.98b9.37038
Waibel, F. W. A., & Böni, T. (2022). Nonoperative Treatment of Charcot Neuro-osteoarthropathy. Foot and Ankle Clinics, 27(3), 595-616. https://doi.org/https://doi.org/10.1016/j.fcl.2022.05.002
Wukich, D. K., Sung, W., Wipf, S. A. M., & Armstrong, D. G. (2011). The consequences of complacency: managing the effects of unrecognized Charcot feet. Diabetic Medicine, 28(2), 195-198. https://doi.org/https://doi.org/10.1111/j.1464-5491.2010.03141.x