
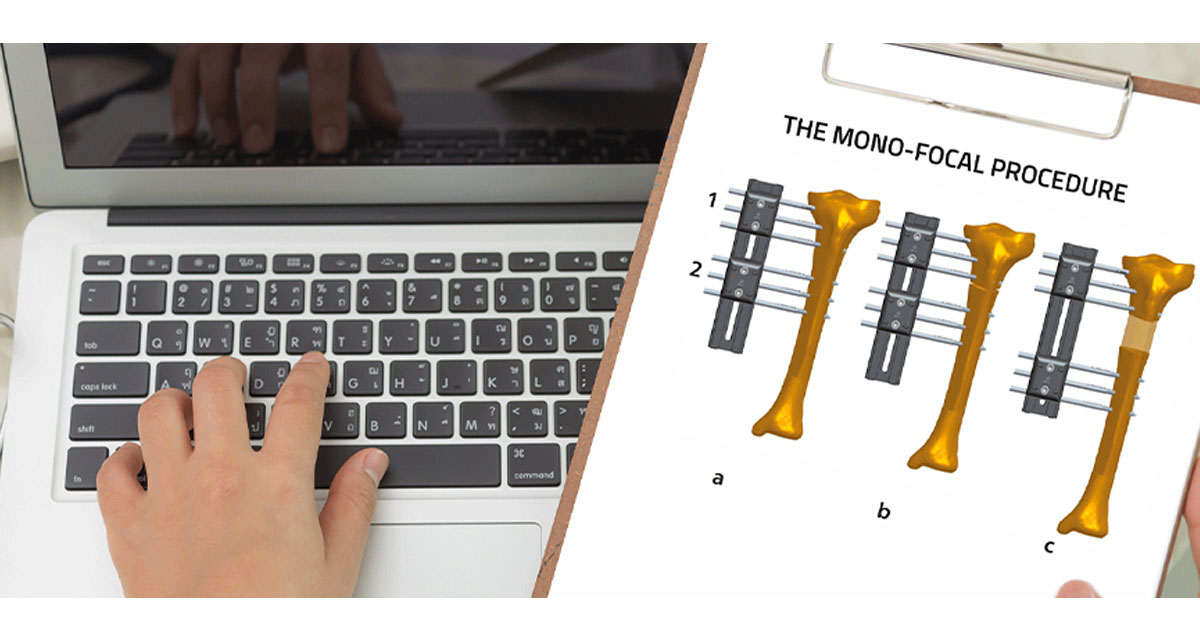
The monofocal procedure is performed for lengthening at a single osteotomy site, for deformity correction with or without lengthening, and when increased stability is required. This procedure may be also used in bone and soft tissue defects when the bone loss is less than 2cm.
The monofocal procedure may be used for bone and soft tissue defects when the bone loss is less than 2cm – the two bony segments next to the defect are transported toward each other, which may cause limb shortening.(1) This technique is also useful in the treatment of hypertrophic nonunions that may be treated by distraction with correction of angulation and shortening.(2)
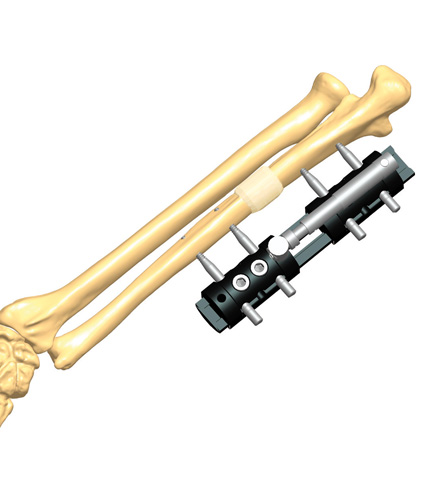
Additionally, the monofocal procedure – e.g. using a monolateral external fixator such as the Limb Reconstruction System (LRS) by Orthofix, which consists of an assembly of clamps, usually two or three, that can slide on a rigid rail and can be connected by compression-distraction units – may be further applied (with two clamps) for lengthening at a single osteotomy site with the callotasis technique.(3)
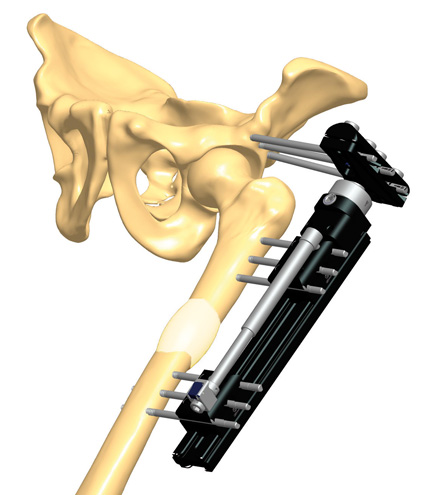
The monofocal procedure for lengthening is indicated in very short bone segments, where the possible smallest distance between proximal and distal clamps is required. The procedure is also indicated for lengthening over 10cm, and in femoral lengthening in pediatric patients or individuals with short stature or limb discrepancies. In femoral lengthening, the fixator’s distal clamp must be placed as far as possible from the knee to preserve joint function.
The monofocal procedure with LRS is recommended for lengthening combined with valgus or varus deformity correction by using progressive correction clamps (e.g. the swivelling clamp or T-Garches clamp) or in case of acute deformity correction with or without lengthening using acute correction templates.
A bone deformity can be corrected acutely or progressively, depending on the site, quality of the bone and tension generated in the soft tissues and nerves. Progressive correction of the bone deformity is indicated when soft tissue and nerve complications may be anticipated, when further surgery is contraindicated, when better accuracy of the correction is needed, or when the deformity occurs during treatment and correction may be managed without any further surgery.
The technique can be effectively used to manage problems at a single focus where additional stability is required – e.g. in the presence of fractures, malunions or nonunions. Regarding the LRS device, the absence of ball-joints, the closer proximity of the screws to the fracture site, and the positioning of the clamps at appropriate points along the entire segment guarantee increased stability. This method is particularly useful for hypertrophic non-union with shortening, which can be managed by distraction.(4)
References
- Po-Hsin C, Hsi-Hsien L et al. 2017. Staged protocol for the treatment of chronic femoral shaft osteomyelitis with Ilizarov’s technique followed by the use of intramedullary locked nail, J Chin Med Ass; 80(6)
- Saleh M, Royston S 1996. Management of nonunion of fractures by distraction with correction of angulation and shortening.
- Aldegheri R. Renzi Brivio L et al. 1989. The Callotasis method of Limb Lengthening. Clin Orthop; 241: 137-45.
- Saleh M 1992. Non-union Surgery. Part I. Basic Principles of management. Int J Orthop Trauma; 2:4-18.




